Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 2
Open Access
Volume 2
Casper Poulsen1; Joakim L Lindhart2,3; Hans Henrik Nielsen3,4; Mikkel Rindom3,4
*Corresponding Author: Casper Bo Poulsen
Faculty of Health Science, Aarhus University, Vennelyst Boulevard 4, 8000 Aarhus, Denmark.
Tel: +45-28557730, Email: Casppu@rm.dk
Article Info
Received: Sep 16, 2022
Accepted: Oct 22, 2022
Published: Oct 31, 2022
Archived: www.jclinmedsurgery.com
Copyright: © Poulsen CB (2022).
Abstract...
A 75-year-old woman treated for T3N0M0 nodular basal cell carcinoma on the nose with erosion. Plastic surgeons reconstructed a total rhinectomy defect with a free flap. Pre surgery CT scans was used in collaboration with in-house 3D engineers to regenerate a mirrored image for the anaplastologists to create the prosthesis.
Keywords: Nose reconstruction; Reconstructive surgery; Plastic Surgery; 3D Visualization; 3D
Technology; Cancer
Abbreviations: BCC: Basal Cell Carcinoma; 3D: Three Dimensional; MRI: Magnetic Resonance
Imaging; CT: Computed Tomography; ENT: Ear, Nose, and Throat; RFFF: Radial Forearm Free Flap;
HU: Hounsfield UNIT.
Citation: Poulsen CB, Lindhart JL, Nielsen HH, Rindom M. 3D-Aided Manufacturing of Nose Prosthesis after Total Rhinectomy. J Clin Med Surgery. 2022; 2(2): 1052.
Introduction
Basal Cell Carcinoma (BCC) is the most common type of carcinoma worldwide. In many countries BCCs are not included due to the low mortality rate [1]. BCC incidence in the United States, is estimated to be 4.3 million cases each year based on data from insurance registries and official diagnosis statistics [2]. Incidence of BCCs appear far more often in the Caucasian population and is related to geographic place of residence, highest incidence near equator, since ultraviolet exposure is associated with evolvement of BCC [3].
Multidisciplinary collaboration between engineers and surgeons using Three-Dimensional (3D) printing in a broad range of settings are a rapidly emerging field with growing interest in different surgical aspects [4]. Currently the use of 3D printing and processing of personal radiological imaging of patients have shown to be effective in pre-operative planning of surgery and intra-operative navigation as well as surgical training and patient education [5,6]. The use of 3D printed models has shown improvement of surgical accuracy as well as reduction of surgical duration, since it improves visualization of anatomical structures compared to two-dimensional data [5]. Despite the growth of implementing 3D in surgical planning, to our knowledge, this paper is the first do describe patient personalized 3D printing and planning for post-operative facial aesthetic appearance using nose prosthesis. We present the following case in accordance with the CARE reporting checklist. Written consent for publication has been obtained from the patient.
Case report
A 75-year-old woman was recently referred from her general practitioner to the Department of Plastics and Breast Surgery at the Aarhus University Hospital with a neglected tumor on the nose. In 2015 the patient had been diagnosed with T3N0M0 nodular BCC on the left ala nasi. She was evaluated and offered surgical excision and reconstruction as primary treatment but initially rejected this. Instead, the tumor was treated with electron beam radiotherapy, with a total dosage of 54Gy in 18 fractions. This induced complete remission of the tumor but at checkup three months after the treatment the patient presented with ulceration in the radiation scar and a punch biopsy confirmed local recurrence. She was recommended surgical intervention, but the patient declined any further treatment at this point. Five years later in 2020 she was referred to our department for reevaluation of the tumor site. She now presented with a large ulcer on the nose that had eroded the left side with complete loss of the left ala nasi (Figure 1). Tumor mapping with punch biopsies confirmed that the tumor had also infiltrated part of the left cheek, the dorsum nasi and the columella. Magnetic Resonance Imaging (MRI) and Computed Tomography (CT) scans were performed and revealed no involvement of the facial bones or the surrounding soft tissues. Due to the widespread tumor growth the patient was recommended total rhinectomy. The surgical removal of the tumor was performed by an Ear, Nose and Throat (ENT) surgeon with a 2 cm margin. The resection included the whole outer nose, the septum nasi, left inferior nasal conchae, spina nasi, part of the soft tissue on the left chin as well as the skin on the upper lip. Frozen section procedure was performed and confirmed complete interoperative resection. Simultaneous with the rhinectomy, plastic surgeons raised a free sub fascial Radial Forearm Free Flap (RFFF), measuring approximately 7 x 7 cm with an 8 cm vascular pedicle. The radial forearm free flap was then transferred to the defect and anastomosed to the left facial vessels. The vascular pedicle was passed via a subcutaneous tunnel to the recipient vessels and end-to-end anastomoses were performed using a microscope. Total time of ischemia was 64 minutes. Flap perfusion was monitored using a handheld doppler ultrasound device. At the center of the flap an 8 mm internal silicon tube was inserted to establish nasal airflow (Figure 2). The flap donor site was covered with full-thickness skin graft from the upper arm.
The post-operative course was uneventful, and no complications were observed during the hospital admission. The patient was discharged nine days postoperatively. Since the aim of the procedure was not to make a full nasal reconstruction, but instead a personalized prosthesis, a 3D blueprint (Figure 3) was performed to visualize the shape and size of the nose pre-operatively in close relation with the 3D engineer. This 3D blueprint was created using the already existing preoperative CT scan. To discriminate soft tissue and bone, the 3D model is reconstructed using the different Hounsfield Unit (HU) for soft tissue as well as bone. HU for bones were set to 226 HU to 3071 HU and values for soft tissue were -700 to 225 HU. Since the right side of the nose was not affected cosmetically, this side was mirrored to create a visual template model for the whole nose by the 3D engineer. By utilizing the mirror image of the patient’s healthy right side of the nose to cover the defect as seen in Figure 4, we were able to create an accurate model of how the healthy nose would have appeared in its entirety. This template model was used to shape and visualize the nose for the anaplastologist, to create the personalized prosthesis for the final look of the patient. A glued prosthesis was chosen for this patient and the result one year postoperative is shown in Figure 5. The patient was offered a minor revision of the left sided nasolabial flap but declined.

Figure 1: Preoperative T3N0M0 nodular BCC tumor on the nose
showing loss of left ala nasi. This image is published with the patients consent.

Figure 2: Postoperative result after total rhinectomy with radial
forearm free flap.
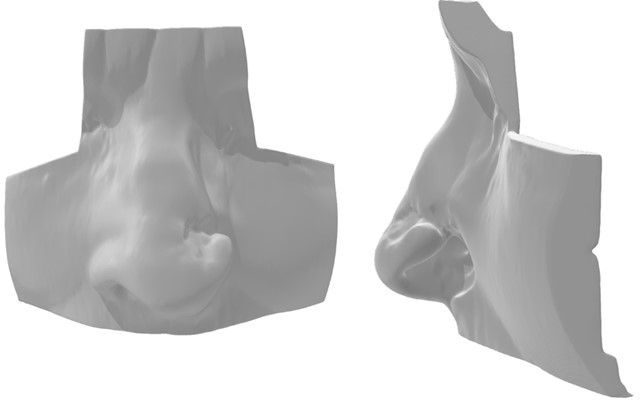
Figure 3: Preoperative 3D figure of the soft tissue defect.
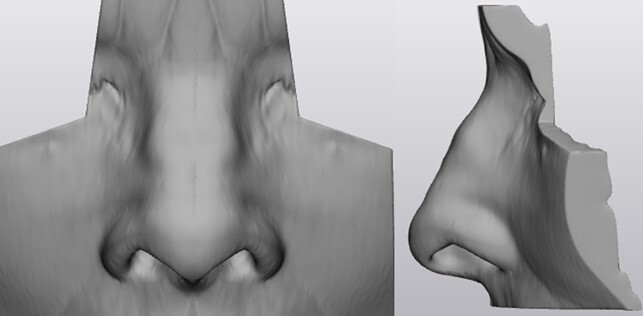
Figure 4: 3D mirrored model of the healthy right side of the
nose.

Figure 5: 12 months postoperative result with prosthesis made
from the mirrored image in Figure 4. This image is published with
the patients consent.
Discussion
While total nasal reconstruction often is the primary choice of treatment to reach a functional as well as aesthetically acceptable result after total rhinectomy, some patients would not be able to go through the multistep surgery needed for this. In our case a total rhinectomy followed up with a prosthesis, was the choice of treatment since partial rhinectomy of the left part of the nose would lead to a difficult multistep reconstruction, of which the patient might not survive or have severe complications due to comorbidities. The use of aesthetic prosthetics to replace the defect post-rhinectomy is widely known [7].
We present an extensive facial nodular BCC case showing the important collaboration between 3D engineers, surgeons, and an anaplastologist in a multidisciplinary team, to conquer difficult and rare patient cases to accomplish the best possible result for the patients. The collaboration with engineers and 3D printing and imaging is an emerging subject that continues to push the boundaries of surgical and medical achievements in recent years and years to come [4-6]. 3D printing does not cause any additional harm to the patient since the 3D imaging can be made using former CT and MRI scans the patient undergoes during pre-operative examinations and thus, no additional radiation exposure for patients. We used an in-house 3D printing department which on one side has the advantage of close relation to the surgeons, as well as easy access to convertible imaging from scans and fast production of 3D imaging and printing. The use of in-house printing saves both time as well as not jeopardizing the legal part of protecting patient sensitive data. A 3D engineering department has on one side the disadvantage of being an extra cost in the short-term for the hospital, whereas the long-term integration of 3D printing in surgery has been shown to be a cost reductive option for the departments because of the better planning of procedures. The growing interest of 3D printing with constantly expanding fields might justify the cost, to create the best patient personalized planning of interventions [8]. The use of 3D printing does not delay the treatment of the patient since the printing is performed parallel to the normal planning of intervention.
The use of 3D printing for pre-operational as well as intra-operative planning is widely known, but the use of post-operative assessment for aesthetic appearance is not well documented [4-6]. Utilizing a 3D printed face with a mirrored right nose covering the left defect nose in combination with pre-operative images, the anaplastologist managed to create an aesthetic nasal prosthesis personalized for the patient to match the former healthy nose aesthetically as closely as possible. By using a 3D printed model anaplastologist can easily visualize the geometry of the nose compared to the standard use of images. In case of patients who do not meet the criteria for the extensive multistep total nasal reconstruction, prosthetic advancement for replacement of nasal features have resulted in an aesthetically accepted solution [7,9]. Soon 3D printing in material that both visually as well as tactile imitates normal skin might be possible, leading to better 3D printed models.
Benefits from the use of nasal prosthesis include faster recovery due to the less extensive surgery leading to faster discharge. The use of nasal prosthetics requires an experienced anaplastologist to manage the specific defects [7]. The disadvantages using nasal prosthesis includes the technically challenging production process with regards to esthetics and fit, and the trouble from daily use and regular cleaning. Another disadvantage compared to total nasal reconstruction is the need for replacement of the prosthesis on average every 2 years [9].
We presented a case showing the beneficial use of 3D engineers from our in-house department in the post-operative planning of an acceptable aesthetic outcome in a comorbid patient undergoing total rhinectomy as part the treatment of an extensive nodular BCC. This technique meets the growing demand of patient personalized solutions, that can be accomplished in a multidisciplinary team between surgeons, engineers and anaplastologists using the emerging field of 3D imaging and printing. However, this approach is not necessarily the best solution for all patients, but it expands the opportunities for aesthetic facial reconstructions.
Declarations
Statement and Declarations: The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
The authors have no relevant financial or non-financial interests to disclose.
Ethics: The authors are accountable for all aspects of the work presented in this paper. The procedures performed were in accordance with the ethical standards of the institutional and national research committees and with the Helsinki Declaration. Written informed consent was obtained from the patient fo publication of this case report and accompanying images.
References
- Rogers HW, Weinstock MA, Feldman SR. Incidence Estimate of Nonmelanoma Skin Cancer (Keratinocyte Carcinomas) in the U.S. Population, 2012. JAMA Dermatol. 2015; 151: 1081-1086.
- Skin Cancer Foundation Skin Cancer Facts. 2020.
- Verkouteren JAC, Ramdas KHR, Wakkee M, Nijsten T. Epidemiology of basal cell carcinoma: scholarly review. Br J Dermatol. 2017; 177: 359-372.
- Pugliese L, Marconi S, Negrello E, Mauri V, Peri A, et al. The clinical use of 3D printing in surgery. Updates Surg. 2018; 70: 381- 388.
- Ogunleye AA, Deptula PL, Inchauste SM, Zelones JT, Walters S, et al. The utility of three-dimensional models in complex microsurgical reconstruction. Arch Plast Surg. 2020; 47: 428-434.
- Marconi S, Pugliese L, Botti M, Peri A, Cavazzi E, et al. Value of 3D printing for the comprehension of surgical anatomy. Surg Endosc. 2017; 31: 4102-4110.
- Scolozzi P, Jaques B. Treatment of midfacial defects using prostheses supported by ITI dental implants. Plast Reconstr Surg. 2004; 114: 1395-1404.
- Martelli N, Serrano C, van den Brink H, Pineau J, Prognon P, et al. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery. 2016; 159: 1485-1500.
- Becker C, Becker AM, Dahlem KKK, Offergeld C, Pfeiffer J, et al. Aesthetic and functional outcomes in patients with a nasal prosthesis. Int J Oral Maxillofac Surg. 2017; 46: 1446-1450.