Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 5
Open Access
Volume 5
Zhao Qiang1*#; Li Xing-Guang2#
*Corresponding Author: Zhao Qiang
Center for Precion Medicine and Translational Research, Tianjin Cancer Hospital Airport Hospital, Tianjin 300000, China.
Email: zq2143740@126.com
Article Info
Received: Jun 20, 2025
Accepted: Jul 30, 2025
Published: Aug 06, 2025
Archived: www.jclinmedsurgery.com
Copyright: © Qiang Z (2025).
Abstract...
Immunotherapy has revolutionized the management of cancer treatment, together with encouraging clinical outcomes. Instead, increasing experimental trials has demonstrated that conventional Immune Checkpoint Inhibitors (ICIs) present low efficiency in a large proportion of patients with many cancer types, usually accompanied by serious adverse events. The investigation of neoantigen opens up a new field of tumor immunotherapy, synergistically paving the way for individual immunotherapy. The accuracy and time-efficiency of neoantigens prediction constitute the challenging factor involved in clinical application. This article represents a systematic summary of the history and identification of neoantigen, as well as the challenges in its future development.
Keywords: Neoantigen; Immunotherapy; Individualization; Cancer vaccine; Adoptive cell therapy.
Citation: Qiang Z, Xing-Guang L. Application of neoantigens in personalized cancer immunotherapy. J Clin Med Surgery. 2025; 5(2): 1200.
Introduction
Cancer immunotherapy has ushered in a new era of cancer treatment. Immune Checkpoint Inhibitors (ICIs) targeting PD-1, PD-L1, and CTLA-4 have become the mainstay of cancer immunotherapy and have been widely used in the treatment of various cancers, improving the overall survival rate of cancer patients to some extent [1-9]. However, studies have shown that only 10-40% of cancer patients benefit from ICI treatment, and 20% of them have to interrupt or discontinue treatment due to immune-related side effects, which can even be fatal in severe cases. Therefore, there is an urgent need to deeply understand the intrinsic molecular mechanisms of cancer immunotherapy and develop new immunotherapeutic approaches [1,7-9].
Cancer is a disease caused by DNA damage and gene mutations, and those antigens that are produced by somatic missense mutations, expressed only in tumor cells, and can induce an endogenous T cell immune response are called tumor neoantigens [10-16]. Tumor neoantigens are mainly produced by mutations such as Single Nucleotide Variations (SNVs), gene fusions, alternative RNA splicing, intron retention, DNA insertions/deletions, and post-translational modifications and endogenous retroviruses can also produce such antigens [17,18].
The development of Next-Generation Sequencing (NGS) technology has revolutionized the identification of tumor neoantigens, and there is evidence that tumor neoantigens are dual targets of endogenous antitumor immune response and cancer immunotherapy [1,4-10,19]. Tumor mutational burden (TMB, a commonly used surrogate marker of tumor neoantigens) is related to the number of tumor-infiltrating lymphocytes and the survival rate of cancer patients. In addition, TMB is an important biomarker for evaluating the response to ICI treatment. Studies have shown that two neoantigen-based cancer treatments, personalized vaccines and adoptive immune cell therapy, have shown good antitumor effects in the clinic. Therefore, the identification and application of tumor neoantigens will have important value for the clinical treatment of tumors [20].
The development of NGS and bioinformatics technologies has made the rapid identification of tumor neoantigens possible, providing a cost-effective method for personalized cancer immunotherapy. However, only a small fraction of the neoantigens predicted by existing technologies and methods have been confirmed to induce immune responses. Therefore, the existing neoantigen prediction methods still have great limitations, and the clinical application and translation based on neoantigens face great challenges [2-16]. This paper mainly discusses the history of tumor neoantigens, their identification methods, their applications in cancer immunotherapy, and the challenges they face.
History of tumor neoantigens
The earliest cancer immunotherapy can be traced back to the mid-20th century. Gross reported that transplantable tumors can induce active immunity in syngeneic mice [21]; Foley’s study showed that carcinogen-induced tumors are antigenic and can be recognized by the immune system [22]; De Plaen et al. discovered the first new antigen recognized by Cytotoxic T Lymphocytes (CTLs) in a Methylcholanthrene (MCA)-induced mouse tumor model [23]; Monach et al. found that CD4+ T cells can induce a specific antitumor immune response and inhibit tumor growth after recognizing tumor neoantigens [24]; Robbins et al. discovered new antigens recognized by TumorInfiltrating Lymphocytes (TILs) and CTLs in human melanoma and renal cell carcinoma, respectively [25,26]; Huang and his colleagues found that melanoma patients’ tumors almost completely disappeared after receiving autologous TILs [27]; Lennerz et al. found that T lymphocytes play a major role in the antitumor immune response induced by neoantigens in a longterm surviving melanoma patient [28]; Zhou et al. found in a study on melanoma patients that adoptive TILs were associated with tumor regression and could persist in tumor patients for a long time [29]; in 2008, Ley et al. used NGS technology for tumor neoantigen identification research, and more tumor neoantigens can be found by comparing the genomic mutations of tumor and normal tissues, which greatly promoted the research of tumor neoantigens [30]; Castle et al. used NGS technology to evaluate the antitumor activity of neoantigen vaccines in the B16 melanoma model [31]; Robbins et al. found that NGS helps identify neoantigens that can induce TILs response in melanoma patients [32]; Gubin et al. identified neoantigens as a target for ICI treatment in a sarcoma mouse model [33]; Tran et al. found that in metastatic epithelial cancer, adoptive CD4+ T against specific antigens has significant antitumor activity and causes tumor regression [34]; Chan and Rizvi et al. confirmed in melanoma and lung cancer patients that neoantigen load is related to the clinical therapeutic effect of ICIs [35,36]; in 2015, Beatriz’s team reported for the first time that neoantigen vaccines could enhance T cell immune response in advanced melanoma patients, and at the same time proved the efficacy and feasibility of personalized dendritic cell vaccines [37]; Tran and his colleagues found that adoptive cell therapy targeting KRAS neoantigens in advanced colon cancer patients can cause tumor regression [38]; McGranahan et al. found that neoantigen load is correlated with the clinical therapeutic effect of ICIs [39]; Ott et al. achieved significant results in melanoma patients using a peptide vaccine targeting 20 neoantigens, and further demonstrated that personalized neoantigen vaccines combined with nivolumab were effective in advanced solid tumor patients [40].
Identification of neoantigens
Currently, there are two main methods for identifying neoantigens: 1) Direct identification of peptide-MHC complexes (Figure 1) [1-9,41,42]; 2) Prediction of neoantigens by NGS technology combined with bioinformatics methods (Figure 2) [1-9,41,42].
Direct identification of peptide-MHC complexes [6,8,20,24,43-46]
MHC class I and class II molecules are mainly responsible for the presentation of intracellular neoantigens, and Mass Spectrometry (MS) technology can be used to detect peptides/ligands bound to MHC molecules, so that neoantigens can be directly identified. This method can not only identify neoantigens during the presentation process, but also identify neoantigens produced by the post-translational modification process. The development of high-throughput MS technology has greatly promoted the identification of neoantigens. However, direct identification methods based on MS technology have great limitations. The collection and identification of peptides/ligands is very time-consuming and laborious, often taking weeks or even months, which greatly limits their clinical translation and application; in addition, only a small fraction of all peptide/MHC complexes can induce immune responses, resulting in the identification process requiring a large number of tissues and high analysis depth, so this method is mostly used in cell lines and preclinical models, while less in clinical applications.
Prediction of neoantigens by NGS technology combined with bioinformatics methods
In view of the limitations of direct identification methods for neoantigens, the development of NGS and bioinformatics technologies has provided new optional methods for the identification of neoantigens. NGS technology has greatly reduced the cost and cycle of gene sequencing. With the help of NGS technology, we can obtain tumor genomic mutation information, which provides a basis for the identification of neoantigens [42]. The prediction of neoantigens based on NGS and bioinformatics technology mainly includes three steps [1-9,12-15]:
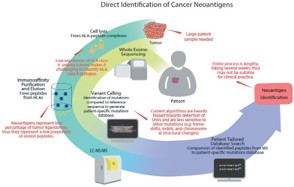
Figure 1: Direct identification of cancer neoantigens [19].
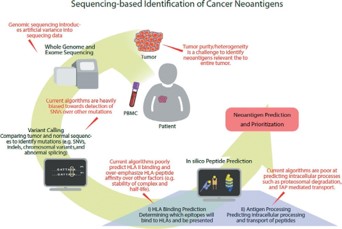
Figure 2: Sequencing-based identification of cancer neoantigens [19].
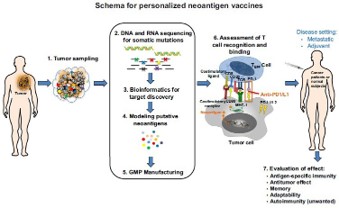
Figure 3: Schema for generating personalized neoantigen vaccines [1].

Figure 4: Combinatorial approaches to generate the adoptive T cell therapy [55].
1) Identification of tumor-specific mutations by Whole-Genome Sequencing (WGS), Whole-Exome Sequencing (WES), or transcriptome sequencing (RNA-seq); 2) Using bioinformatics methods to predict the type of Major Histocompatibility Complex (MHC)/Human Leukocyte Antigen (HLA); 3) Selection of neoantigens.
Using WES results, the genomes of tumor tissue and paired normal tissue are compared to map the DNA mutation spectrum of tumor cells. Combined with RNA-seq results, we can infer which mutated genes are expressed in tumor cells and are likely to become neoantigens. Combining MS and WES can make the prediction of neoantigens more effective [42]. First, tumor-specific gene mutations are identified using WES technology, and a tumor genome mutation library is constructed; then, the peptides identified by LC-MS/MS are compared with the tumor genome mutation library to more accurately identify the neoantigens that can bind to MHC [19,42,47-50].
It is worth noting that the development of bioinformatics has greatly improved the accuracy and effectiveness of tumor neoantigen identification. MHC class I and class II molecules process and present antigens in different ways. The length of peptides bound by MHC-I molecules is usually only 8-10 amino acids, while MHC-II molecules can bind to peptides with a length of 11-20 amino acids [42]. Some bioinformatics tools based on sequencing data such as WES, WGS, and RNA-seq can predict MHC alleles [42,51], such as Optitype and Polysolver, which can predict MHC class I molecules, and seq2HLA, Athlates, HLAscan, HLAProfiler, PHLAT, and ArcasHLA, which can predict both MHC class I and class II molecules. In addition, NetMHC, NetMHCpan, and MHCflurry based on bioinformatics methods have also been used for the identification of neoantigens. The affinity between peptides and MHC and the expression level of mutated genes are important bases for neoantigen identification.
Identification of neoantigen immunogenicity
The generation of neoantigens must meet two conditions:
1) The peptide expressed by the mutated gene must be able to be processed and presented by MHC molecules; 2) The peptide-MHC complex must be recognized by endogenous T cells [4-8,27-29]. MS, NGS, and bioinformatics methods provide a reliable basis for the identification of neoantigens, but whether the screened neoantigens can induce a T cell immune response is another problem that needs to be solved in the process of neoantigen identification [27-29]. In this regard, T cell experiments can determine whether neoantigens presented by MHC can be recognized by T cells and induce subsequent immune responses. Methods such as fluorescently labeled HLA tetramers or multimers and enzyme-linked immunospot (ELISpot) have been used for T cell experiments, but these cell-based assays that play an important role in the identification of neoantigens are often expensive and time-consuming and technically challenging [52].
Clinical application of tumor neoantigens
Tumor-specific vaccines and adoptive immunotherapy are two important applications of neoantigens in individualized tumor immunotherapy:
Tumor-specific vaccines
The concept of tumor neoantigen vaccines was first proposed in the 1990s, and its development largely benefited from the development of high-throughput sequencing technology and bioinformatics. Vaccines based on tumor neoantigens have a wide range of applications in the clinical treatment of tumors. Such vaccines can stimulate the body to produce a specific immune response, and specifically kill tumor cells without damaging normal human cells. According to the delivery method of the vaccine, tumor-specific vaccines can be divided into: Synthetic Long chain Peptides (SLPs), DNA, RNA, Dendritic Cells (DCs), viruses, and bacteria, etc. [1-12]. Neoantigen vaccines exert their anti-tumor effects by activating the body’s specific T cell immune response, inhibiting the growth of tumor cells or killing tumor cells [27-29]. Tumor-specific vaccines based on neoantigens have achieved good results in a series of clinical trials in melanoma and glioma. The results of these clinical trials indicate that personalized neoantigen vaccines are also feasible for “cold” tumors with low TMB and poor response to ICIs [53,54]. In addition, another neoantigen vaccine based on dendritic cells has also achieved good results in ovarian cancer [42]. A growing number of clinical trial results indicate that tumor-specific vaccines based on neoantigens will be a promising research direction in the clinical treatment of tumors.
Adoptive immunotherapy
Adoptive immunotherapy is another important application of neoantigens in tumor clinical treatment and research besides tumor-specific vaccines. This method refers to the in vitro culture of T cells from donors, and the cultured T cells are returned to the donor’s body to enhance the donor’s own T cell anti-tumor response, thereby killing tumor cells [27-29,42,5559]. The cell types of adoptive T cell therapy include: 1) tumorinfiltrating T cells; 2) T cells genetically engineered to express T Cell Receptors (TCRs) or Chimeric Antigen Receptors (CARs); 3) other immune cells such as natural killer cells. Adoptive T cell therapy has been shown to play an anti-tumor role in gastrointestinal tumors, metastatic cholangiocarcinoma, colorectal cancer, cervical cancer, breast cancer, etc. The results of these clinical trials indicate that adoptive immunotherapy based on neoantigens will play an increasingly important role in tumor immunotherapy [42,55-59].
Prospect
Tumor neoantigens can stimulate endogenous immune responses and enhance the body’s anti-tumor activity, playing an important role in tumor immunotherapy. Direct identification methods of neoantigens based on MS technology are relatively effective, but they are time-consuming and laborious, which limits their clinical application. The development of NGS and bioinformatic technology not only enables us to quickly obtain genomic mutation and expression information, but also to predict the type/genotype of MHC [4,7,8,11,43-46]. Although the development of NGS and bioinformatics technology has greatly promoted the identification of neoantigens and its clinical translation and application, the accuracy of its prediction still has a lot of room for optimization [1-10,52].
Despite the great progress in tumor vaccine research based on neoantigens, its development still faces many challenges, among which the identification of neoantigen immunogenicity is a major obstacle; due to the existence of tumor heterogeneity, neoantigens are expressed in different tumors, Different parts of the same tumor are different, which also causes great trouble for the design of neoantigen vaccines and their transportation and delivery in the body; tumor cells themselves can evolve the ability to avoid immune cell recognition and attack [8,12,14-19]. With the continuous development of new technologies, research on neoantigens in tumors will continue to deepen, and immunotherapy based on neoantigens in tumors will inevitably have broader application prospects in the clinical treatment of tumors.
Declarations
Conflict of interest: The authors declare that there is no conflict of interest.
Acknowledgements: We acknowledge the funding support from the Tianjin Health Science and Technology Project (Project Number: RC20189) from China.
References
- Ma W, Pham B, Li T. Cancer neoantigens as potential targets for immunotherapy. Clinical & Experimental Metastasis. 2021: 1–10.
- Yu G, He X, Li X, et al. Driving neoantigen-based cancer vaccines for personalized immunotherapy into clinic: a burdensome journey to promising land. Biomedicine & Pharmacotherapy. 2022; 153: 113464.
- Lybaert L, Lefever S, Fant B, et al. Challenges in neoantigen-directed therapeutics. Cancer Cell. 2023.
- Katsikis PD, Ishii KJ, Schliehe C. Challenges in developing personalized neoantigen cancer vaccines. Nature Reviews Immunology. 2023: 1–15.
- Gupta RG, Li F, Roszik J, et al. Exploiting tumor neoantigens to target cancer evolution: current challenges and promising therapeutic approaches. Cancer Discovery. 2021; 11: 1024–39.
- Okada M, Shimizu K, Fujii S. Identification of neoantigens in cancer cells as targets for immunotherapy. International Journal of Molecular Sciences. 2022; 23: 2594.
- Reynolds CR, Tran S, Jain M, et al. Neoantigen cancer vaccines: generation, optimization, and therapeutic targeting strategies. Vaccines. 2022; 10: 196.
- Li X, You J, Hong L, et al. Neoantigen cancer vaccines: a new star on the horizon. Cancer Biology & Medicine. 2023.
- Fang X, Guo Z, Liang J, et al. Neoantigens and their potential applications in tumor immunotherapy. Oncology Letters. 2022; 23: 1–9.
- Wolf Y, Sameuls Y. Neoantigens in cancer immunotherapy: quantity vs. quality. Molecular Oncology. 2023; 17: 1457–9.
- Zhang Q, Jia Q, Zhang J, et al. Neoantigens in precision cancer immunotherapy: from identification to clinical applications. Chinese Medical Journal. 2022; 135: 1285–1298.
- Zheng Y, Fu Y, Wang PP, et al. Neoantigen: a promising target for the immunotherapy of colorectal cancer. Disease Markers. 2022; 2022.
- Komuro H, Shinohara S, Fukushima Y, et al. Single-cell sequencing on CD8+ TILs revealed the nature of exhausted T cells recognizing neoantigen and cancer/testis antigen in non-small cell lung cancer. Journal for Immunotherapy of Cancer. 2023; 11.
- Capietto AH, Hoshyar R, Delamarre L. Sources of cancer neoantigens beyond single-nucleotide variants. International Journal of Molecular Sciences. 2022; 23: 10131.
- Shang S, Zhao Y, Qian K, et al. The role of neoantigens in tumor immunotherapy. Biomedicine & Pharmacotherapy. 2022; 151: 113118.
- Pao SC, Chu MT, Hung SI. Therapeutic vaccines targeting neoantigens to induce T-cell immunity against cancers. Pharmaceutics. 2022; 14: 867.
- Linnemann C, Mezzadra R, Schumacher TNM. TCR repertoires of intratumoral T-cell subsets. Immunological Reviews. 2014; 257: 72–82.
- Srivastava RM, Purohit TA, Chan TA. Diverse neoantigens and the development of cancer therapies. Seminars in Radiation Oncology. 2020; 30: 113–28.
- Chen I, Chen MY, Goedegebuure SP, et al. Challenges targeting cancer neoantigens in 2021: a systematic literature review. Expert Review of Vaccines. 2021; 20: 827–37.
- Jiang T, Shi T, Zhang H, et al. Tumor neoantigens: from basic research to clinical applications. Journal of Hematology & Oncology. 2019; 12: 1–13.
- Gross L. Intradermal immunization of C3H mice against a sarcoma that originated in an animal of the same line. Cancer Research. 1943; 3: 326–33.
- Foley EJ. Antigenic properties of Methylcholanthrene-induced tumors in mice of the strain of origin. Cancer Research. 1953; 13: 835–7.
- De Plaen E, Lurquin C, Van Pel A, et al. Immunogenic (tum-) variants of mouse tumor P815: cloning of the gene of tum-antigen P91A and identification of the tum-mutation. Proceedings of the National Academy of Sciences. 1988; 85: 2274–2278.
- Monach PA, Meredith SC, Siegel CT, et al. A unique tumor antigen produced by a single amino acid substitution. Immunity. 1995; 2: 45–59.
- Robbins PF, El-Gamil M, Li YF, et al. A mutated beta-catenin gene encodes a melanoma-specific antigen recognized by tumor infiltrating lymphocytes. Journal of Experimental Medicine. 1996; 183: 1185–92.
- Brändle D, Brasseur F, Weynants P, et al. A mutated HLA-A2 molecule recognized by autologous cytotoxic T lymphocytes on a human renal cell carcinoma. Journal of Experimental Medicine. 1996; 183: 2501–8.
- Huang J, El-Gamil M, Dudley ME, et al. T cells associated with tumor regression recognize frameshifted products of the CDKN2A tumor suppressor gene locus and a mutated HLA class I gene product. The Journal of Immunology. 2004; 172: 6057–64.
- Lennerz V, Fatho M, Gentilini C, et al. The response of autologous T cells to a human melanoma is dominated by mutated neoantigens. Proceedings of the National Academy of Sciences. 2005; 102: 16013–8.
- Zhou J, Dudley ME, Rosenberg SA, et al. Persistence of multiple tumor-specific T-cell clones is associated with complete tumor regression in a melanoma patient receiving adoptive cell transfer therapy. Journal of Immunotherapy. 2005; 28: 53.
- Ley TJ, Mardis ER, Ding L, et al. DNA sequencing of a cytogenetically normal acute myeloid leukaemia genome. Nature. 2008; 456: 66–72.
- Castle JC, Kreiter S, Diekmann J, et al. Exploiting the mutanome for tumor vaccination. Cancer Research. 2012; 72: 1081–91.
- Robbins PF, Lu YC, El-Gamil M, et al. Mining exomic sequencing data to identify mutated antigens recognized by adoptively transferred tumor-reactive T cells. Nature Medicine. 2013; 19: 747.
- Gubin MM, Zhang X, Schuster H, et al. Checkpoint blockade cancer immunotherapy targets tumour-specific mutant antigens. Nature. 2014; 515: 577–81.
- Tran E, Turcotte S, Gros A, et al. Cancer immunotherapy based on mutation-specific CD4+ T cells in a patient with epithelial cancer. Science. 2014; 344: 641–5.
- Chan TA, Wolchok JD, Snyder A. Genetic basis for clinical response to CTLA-4 blockade in melanoma. New England Journal of Medicine. 2015; 373: 1984.
- Rizvi NA, Hellmann MD, Snyder A, et al. Mutational landscape determines sensitivity to PD-1 blockade in non–small cell lung cancer. Science. 2015; 348: 124–8.
- Carreno BM, Magrini V, Becker-Hapak M, et al. A dendritic cell vaccine increases the breadth and diversity of melanoma neoantigen-specific T cells. Science. 2015; 348: 803–8.
- Tran E, Robbins PF, Lu YC, et al. T-cell transfer therapy targeting mutant KRAS in cancer. New England Journal of Medicine. 2016; 375: 2255–62.
- McGranahan N, Furness AJS, Rosenthal R, et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science. 2016; 351: 1463–9.
- Ott PA, Hu Z, Keskin DB, et al. An immunogenic personal neoantigen vaccine for patients with melanoma. Nature. 2017; 547: 217–21.
- Gubin MM, Zhang X, Schuster H, et al. Checkpoint blockade cancer immunotherapy targets tumour-specific mutant antigens. Nature. 2014; 515: 577-81.
- Zhu Y, Liu J. The role of neoantigens in cancer immunotherapy. Frontiers in Oncology. 2021; 11.
- Yadav M, Jhunjhunwala S, Phung QT, et al. Predicting immunogenic tumour mutations by combining mass spectrometry and exome sequencing. Nature. 2014; 515: 572–6.
- Singh-Jasuja H, Emmerich NPN, Rammensee HG. The Tübingen approach: identification, selection, and validation of tumor-associated HLA peptides for cancer therapy. Cancer Immunology Immunotherapy. 2004; 53: 187–95.
- Bassani-Sternberg M, Bräunlein E, Klar R, et al. Direct identification of clinically relevant neoepitopes presented on native human melanoma tissue by mass spectrometry. Nature Communications. 2016; 7: 1–16.
- Creech AL, Ting YS, Goulding SP, et al. The role of mass spectrometry and proteogenomics in the advancement of HLA epitope prediction. Proteomics. 2018; 18: 1700259.
- Wang Z, Cao YJ. Adoptive cell therapy targeting neoantigens: a frontier for cancer research. Frontiers in Immunology. 2020; 11: 176.
- Schumacher TN, Scheper W, Kvistborg P. Cancer neoantigens. Annual Review of Immunology. 2019; 37: 173–200.
- Li L, Goedegebuure SP, Gillanders WE. Preclinical and clinical development of neoantigen vaccines. Annals of Oncology. 2017; 28: xii11–xii17.
- Josephs TM, Grant EJ, Gras S. Molecular challenges imposed by MHC-I restricted long epitopes on T cell immunity. Biological Chemistry. 2017; 398: 1027–36.
- Rock KL, Reits E, NeeȠes J. Present yourself! By MHC class I and MHC class II molecules. Trends in Immunology. 2016; 37: 724– 37.
- Slota M, Lim JB, Dang Y, et al. ELISpot for measuring human immune responses to vaccines. Expert Review of Vaccines. 2011; 10: 299–306.
- Fritsch EF, Burkhardt UE, Hacohen N, et al. Personal neoantigen cancer vaccines: a road not fully paved. Cancer Immunology Research. 2020; 8: 1465.
- Sahin U, Türeci Ö. Personalized vaccines for cancer immunotherapy. Science. 2018; 359: 1355–60.
- Yamamoto TN, Kishton RJ, Restifo NP. Developing neoantigentargeted T cell–based treatments for solid tumors. Nature Medicine. 2019; 25: 1488–99.
- Xu R, Du S, Zhu J, et al. Neoantigen-targeted TCR-T cell therapy for solid tumors: how far from clinical application. Cancer Letters. 2022: 215840.
- Komuro H, Shinohara S, Fukushima Y, et al. Single-cell sequencing on CD8+ TILs revealed the nature of exhausted T cells recognizing neoantigen and cancer/testis antigen in non-small cell lung cancer. Journal for Immunotherapy of Cancer. 2023: 11.
- Scheper W. The landscape of T cell-recognized neoantigens in cancer patients. Genes & Immunity. 2023; 24: 287–8.
- Guan H, Wu Y, Li LU, et al. Tumor neoantigens: novel strategies for application of cancer immunotherapy. Oncology Research. 2023; 31: 437–48.
- Vivekanandhan S, Bahr D, Kothari A, et al. Immunotherapies in rare cancers. Molecular Cancer. 2023; 22: 23.