Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 5
Open Access
Volume 5
Espiney Amaro C1,2*; Nunes CR2,3; d’Espiney R4; Saraiva J1
*Corresponding Author: Espiney Amaro C
Otorhinolaryngology Unit, and Sleep Unit of Hospital Cuf Descobertas, Portugal, Rua Mário Botas S/N, 1998-018 Lisboa, Portugal.
Tel: 00351-914777966; Email: dicacarla@hotmail.com
Article Info
Received: Jun 19, 2025
Accepted: Jul 22, 2025
Published: Jul 29, 2025
Archived: www.jclinmedsurgery.com
Copyright: © Amaro CE (2025).
Abstract...
Introduction: Obstructive Sleep Apnea (OSA) is a sleep-related breathing disorder characterized by episodes of partial or complete airway collapse resulting in oxygen desaturations and sleep disturbance. The treatment of choice is Continuous Positive Airway Pressure (CPAP) however patients can fail to tolerate this treatment modality. In this case report we demonstrate the importance of undertaking an airway assessment in those demonstrating poor compliance or refractory symptoms with CPAP using Drug Induced Sleep Endoscopy (DISE).
Results: A 42-year-old male presented with moderate OSA with an Apnea/Hypopnea Index (AHI) of 23.4 events per/hour who showed no compliance to prescribed CPAP. Computed Tomography (CT) scan and Drug Induced Sleep Endoscopy (DISE) revealed a deviated septum with nasal valve incompetence, a complete palate obstruction and a prolapsing right corniculate cartilage towards glottic midline resulting in airway obstruction. He underwent a rhinoseptoplasty, lateral Expansion Sphincter Pharyngoplasty (ESP) and suspension laryngeal microsurgery with laser removal of the right corniculate cartilage. Three months following surgery, patient denied snoring and the polysomnography type III showed an improvement in AHI to 7.6 events per/hour.
Conclusion: It is important to recognize the anatomical causes of OSA and in this case report we highlight the benefit of DISE as a diagnostic tool in investigating patients with refractory symptoms despite CPAP. Functional airway assessment demonstrates that OSA is often resulting from obstruction at multiple levels and hence patients need a personalized and individualized management to achieve the best surgical results.
Keywords: Sleep apnea; Corniculate cartilage; DISE; Larynx.
Abbreviations: AHI: Apnea/Hypopnea Index; BMI: Body Mass Index; BIS: Bispectral; BRP: Barbed Reposition Pharyngoplasty; CPAP: Continuous Positive Airway Pressure; CT Scan: Computed Tomography Scan; DISE: Drug Induced Sleep Endoscopy; ESP: Expansion Sphincter Pharyngoplasty; ESRS: European Sleep Research Society; ESS : Epworth Sleepiness Scale; ICSD: International Classification of Sleep Disorders; OSA: Obstructive Sleep Apnea; MAD: Mandibular Advancement Devices; PSG: Polysomnography; VOTE: Velum, Oropharynx, Tongue, Epiglottis.
Citation: Amaro CE, Nunes CR, d’Espiney R, Saraiva J. An unusual cause of sleep apnea and the importance of evaluating the larynx: Clinical case. J Clin Med Surgery. 2025; 5(2): 1198.
Introduction
According to the European Sleep Research Society (ESRS), Obstructive Sleep Apnea (OSA) is a sleep-related breathing disorder [1] that must comply with the diagnostic criteria of the International Classification of Sleep Disorders (ICSD-3) [2]. OSA is characterized by pathophysiological mechanisms which result in multilevel upper airway collapse when the inspiratory transpharyngeal pressure exceeds the pharyngeal dilating muscle action [8]. Polysomnography or home sleep apnea testing are the diagnostic tests commonly used to diagnose OSA in uncomplicated adult patients presenting with signs and symptoms that indicate an increased risk of moderate to severe OSA. In patients with comorbidities and inconclusive preliminary results, polysomnography is recommended [3].
Untreated OSA is associated with several comorbidities such as cardiovascular disease, resistant hypertension, metabolic diseases (diabetes and dyslipidemia), dementia and cancer [47]. OSA treatment can result in improved quality of life, daytime sleepiness together with improvement in associated comorbidities and mortality reduction [4,8,10].
Continuous Positive Airway Pressure (CPAP) is the treatment of choice for OSA as it maintains airway patency [9]. It is a therapy which can be poorly tolerated and non-noncompliance rates of up to 50% can be observed within the first week of treatment [11]. Non-compliance can be a result of psychological factors such as anxiety, claustrophobia and worsening insomnia, or physical factors (mask leaks, skin breakdown and dry throat/ nose) [12]. Advances in CPAP designs such as humidification, pressure generation settings and different mask interfaces are available to individually customize treatment to the patient and improve compliance. It is important to be aware of other treatment modalities in patients non-compliant with CPAP and highlighting weight loss and lifestyle guidance in those where weight may be aggravating symptoms [12,13]. In mild and moderate OSA oral mandibular devices may be used and positional therapy might be effective. Otorhinolaryngological and/or maxillofacial surgery may also be indicated in specific cases [12].
In this case report we highlight the importance of recognizing and investigating anatomical causes of OSA which may be refractory or exacerbate noncompliance with CPAP. It demonstrates an uncommon cause of laryngeal involvement in OSA that might also, be the cause of non-compliance to CPAP.
Materials and methods
Clinical data of a 43 years old male with snoring and OSA symptoms.
Results
A 43-year-old male presented with snoring, nocturnal asphyxiation and sensation of nocturnal vomits. He had no previous surgical history, denied alcohol intake and no smoking history. He had a Body Mass Index (BMI) of 23. He scored 13 on the Epworth Sleepiness Scale (ESS) and the Berlin Questionnaire showed a high risk of underlying OSA. His neck circumference was 39 cm. Polysomnography (PSG) Type 3 revealed moderate OSA with Apnea/Hypopnea Index (AHI) of 23,4 events per hour and when in supine position, AHI was 37 events per hour. Median oxygen saturation was 92% with a minimum oxygen saturation of 82%.
Auto-CPAP therapy was initiated and despite mask adjustments he continued to report significant sleep disturbance on therapy. He was referred to an Ear, Nose and Throat Specialist for further evaluation. On examination found to have a deviated septum, right nasal valve incompetence and rhinitis. He had a IIB grade according to Friedman´s tongue position classification and the tonsils were grade 2 [14]. The Computed Tomography Scan (CT scan) confirmed a deviated septum and sinusitis (Figures 1 & 2). Upper airway CT scan revealed an area of 65.5 mm2, a soft palate with a length of 39 mm and a retroglossal distance of 11.8 mm. It additionally revealed micrognathia, tongue base touching the epiglottis (Figures 3 & 4) and midline prolapse of right arytenoid/vocal fold (Figure 5).
Dynamic assessment of his airway was undertaken by carrying out a Drug Induced Sleep Endoscopy (DISE) with propofol sedation and the depth of sedation was monitored with Bispectral Index (BIS). The VOTE (velum, oropharynx, tongue, epiglottis) classification was used to characterize findings and structures contributing to the degree of obstruction [15]. During DISE, the patient snored, kept his mouth opened and several events resulting in >4% oxygen desaturations where observed. Total anteroposterior velum obstruction (Figure 6) was observed with no opening while performing chin-lift maneuver. Oropharynx lateral walls vibrated, and the tongue base touched the epiglottis but airway obstruction was not observed. Epiglottis had normal configuration and didn’t demonstrate trap door movements. Glottic view showed a prolapse of the right corniculate cartilage towards the midline during inspiration, completely obstructing the airway and causing the apnea events (Figures 7-10).
CPAP was administered on a low continuous positive pressure to maintain the patency of the glottis. Patient remained symptomatic and he maintained non-compliant to CPAP and therefore a surgical approach was performed. He underwent a rhinoseptoplasty with right spreader graft, lateral Expansion Sphincter Pharyngoplasty (ESP) and suspension laryngeal microsurgery with laser with removal of the right corniculate cartilage was undertaken. Three months postoperatively, patient denied snoring, reported improved quality of life and scored 4 on the Epworth Sleepiness Scale. PSG Type III revealed and improved AHI of 7.6 events per/hour and an AHI of 8.7 events per/hour in the supine position. Median oxygen saturation was 95.1% and minimum saturation of 91%.
Discussion
In this case report we highlight the importance of further evaluation of anatomical causes of OSA in patients poorly complaint with CPAP and demonstrating refractory symptoms despite its optimized use. The use of DISE in our patient identified a deviated septum and prolapse of the right corniculate cartilage towards the midline causing complete airway obstruction and resulting in apnea events. A multi-level surgical approach involving the nose, pharynx and larynx allowed an individualized treatment which resulted in symptomatic (absence of snoring and improved quality of life) and objective improvement in AHI and overnight oxygen saturation on repeated PSG.
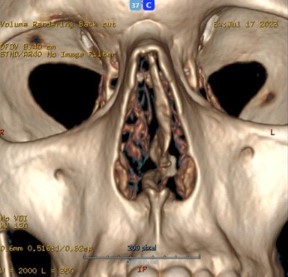
Figure 1: CT scan of the paranasal sinus demonstrated a deviated septum (coronal view).
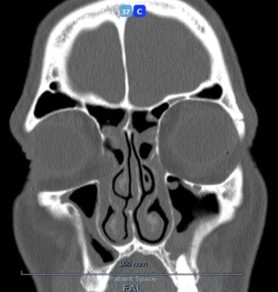
Figure 2: CT scan of the paranasal sinus demonstrating sinusitis.

Figure 3: CT scan of the upper airway demonstrating an area of 65.6 mm2 (axial view).

Figure 4: CT scan of the upper airway demonstrating airway distances: soft palate 39.3 mm; retroglossal 11.8 mm. (Sagittal view). There is also evidence of micrognathia and tongue base touching the epiglottis.
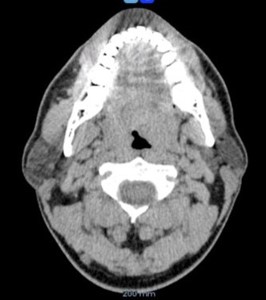
Figure 5: CT scan demonstrating midline prolapse of right arytenoid/vocal fold (Axial view).

Figure 6: DISE: velum complete anteroposterior closure.

Figure 7: DISE image in expiratory time: epiglottic view showing right corniculate cartilage towards midline.

Figure 8: DISE in expiratory time: Glottic view showing right corniculate cartilage towards midline.

Figure 9: DISE in inspiratory time: Epiglottic view showing prolapse to midline of corniculate cartilage, completely closing the airway.
Sleep endoscopy has been tried since 1978 [16,17]. In 1991 at the Royal National Throat, Nose and Ear Hospital in London the use of Drug Induced Sleep Endoscopy (DISE) was pioneered which allowed improved upper airway assessment in a shorter time scale [17]. It is currently used as a diagnostic tool in patients not responding to CPAP therapy as well as improving surgical outcomes for the surgical management of OSA [15,18-20]. Its use in this patient allowed a dynamic and functional upper airway assessment during sleep and detected that the corniculate cartilage prolapse causing almost complete obstruction.
The use of DISE has demonstrated that OSA often results from multilevel obstruction and improved outcomes require an individualized multilevel approach. In patients identified with tongue base and epiglottic collapse the use of Mandibular Advancement Devices (MAD), hypoglossal nerve stimulation or epiglottic surgery can be treatment options for the management of OSA [29-31]. Laryngeal surgery has already been proposed to solve OSA in patients with laryngomalacia, such as, supraglottoplasty [33]. To our knowledge, this is the first case report published where corniculate cartilage removal allowed treatment of it’s prolapse into the airway. This patient also benefitted from a multilevel individualized surgical approach to abnormal nose, pharynx and larynx findings to allow improved post-surgical outcomes.
Nasal breathing contributes to vital physiological functions, such as heating and humidification of inhaled air, and stimulation of ventilation. Nasal obstruction may result in increased collapsibility of the oropharynx and it is frequently observed in patients with OSA [16-18]. Nasal obstruction and sleeping with an opened mouth, have both been identified as causes for nonadherence and failure with CPAP [18,19]. Nasal valve competence should carefully be evaluated by Ear, Nose, Throat specialists as its structure will play an important role in nasal function [17]. In our patient, we undertook a rhinoseptoplasty to correct the deviated septum and nasal valve incompetence as this would allow improved OSA symptoms and likely improved CPAP tolerance if needed in the future.
Surgery in OSA has two main purposes: increase airway area and improve stiffness of the pharyngeal structures. In 1981 Fujita et al introduced the uvulopalatopharyngoplasty as surgical treatment for OSA [25]. Whilst advancements have further improved the surgical technique utilized, not all patients benefit equally from this surgery. This highlights how there can be variability in which structures are resulting in upper airway obstruction and the importance of an individualized dynamic assessment of patients to understand the best surgical management for resolution of symptoms. For example, in patients where palatal obstruction is observed causing OSA they benefit the most from Expansion Sphincter Pharyngoplasty (ESP) and Barbed Reposition Pharyngoplasty (BRP [26-28]. Factors associated with success in pharyngeal surgery have identified as; tonsil size, BMI, AHI, cephalometry and upper airway anatomy [29].
However, and it was possible to identify it mainly because of the introduction of DISE, most cases of OSA have multilevel obstruction demanding a multilevel approach. Tongue base and epiglottic collapse have been identified and treatment with Mandibular Advancement Devices (MAD), hypoglossal nerve stimulation or epiglottic surgery can be proposed [29-31]. The prevalence of epiglottic collapse in OSA is probably higher than it was believed. DISE has helped to diagnose epiglottic collapse allowing its personalized treatment. Epiglottic surgery includes partial epiglottectomy, epiglottopexy and epiglottic stiffening operation [32-35].
Laryngeal surgery has already been proposed to solve OSA in patients with laryngomalacy, such as, supraglottoplasty [33]. However, to our knowledge, prolapsing corniculate cartilage and consequently, corniculate removal to solve glottic occlusion has never been published. Removal of corniculate cartilage has no long-term complications being a safe surgery. Even if OSA didn’t improve and OSA symptoms maintained, corniculate cartilage surgery would probably allow CPAP compliance in this patient.
This patient performed multilevel surgery (nose, pharynx and larynx) with resolution of snoring and a better outcome of OSA. A detailed assessment of the airway allows an individualized treatment ensuring better resolution of OSA.
Conclusion
Surgical assessment of obstructive sleep apnoea has demonstrated that upper airway obstruction are often multileveled. DISE is a diagnostic tool that allows dynamic assessment of the upper airway in a sedated state reflective of natural sleep. It can identify the anatomical structures resulting in obstruction of the upper airway and inform improved surgical decisions for management of OSA. It is a helpful diagnostic tool in evaluating patients who are poorly compliant with CPAP or have refractory symptoms despite optimized CPAP. To our knowledge, this is the first published case revealing the management of prolapsed corniculate cartilage and how an individualized multileveled surgical approach allowed improved patient symptoms and AHI.
References
- Zucconi M, Ferri R. Classification of sleep disorders. In: Bassetti C, McNicholas W, Paunio T, Peigneux P, editors. Sleep Medicine Textbook Second Edition. European Sleep Research Society; 2021: 151–165.
- Medicine AAoS. ICSD-3-Text-Revision-Supplemental-Material.pdf. 2025.
- Maspero C, Giannini L, Galbiati G, Rosso G, Farronato G. Obstructive sleep apnea syndrome: a literature review. Minerva Stomatol. 2015; 64: 97–109.
- Kapur V, Auckley D, Chowdhuri S, Kuhlmann D, Mehra R, Ramar K, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017; 13: 479–504.
- Marin-Oto M, Vicente E, Marin J. Long term management of obstructive sleep apnea and its comorbidities. Multidiscip Respir Med. 2019; 14: 21.
- Balcan B, Uğurlu A. Results of polysomnographies and treatment strategies in elderly patients with symptoms of obstructive sleep apnea syndrome. Turk Thorac J. 2017; 18: 108–113.
- Wang J, Subramanian A, Cockburn N, Xiao J, Nirantharakumar K, Haroon S. Obstructive sleep apnoea syndrome and future risk of dementia among individuals managed in UK general practice. Thorax. 2025; 80: 167–174.
- Qi P, Qi B, Ding Y, Sun J, Gu C, Huo S, et al. Implications of obstructive sleep apnea in lung adenocarcinoma: a valuable omission in cancer prognosis and immunotherapy. Sleep Med. 2023; 107: 268–280.
- Antic N, Catcheside P, Buchan C, Hensley M, Naughton M, Rowland S, et al. The effect of CPAP in normalizing daytime sleepiness, quality of life, and neurocognitive function in patients with moderate to severe OSA. Sleep. 2011; 34: 111–119.
- Akashiba T, Inoue Y, Uchimura N, Ohi M, Kasai T, Kawana F, et al. Sleep apnea syndrome (SAS) clinical practice guidelines 2020. Sleep Biol Rhythms. 2022; 20: 5–37.
- Engleman H, Wild M. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med Rev. 2003; 7: 81–99.
- Goldstein L, Purcell N, Sarmiento K, Neylan T, Maguen S. Barriers to positive airway pressure adherence among veterans with sleep apnea: a mixed methods study. Transl Behav Med. 2022; 12: 870–877.
- Chirinos J, Gurubhagavatula I, Teff K, Rader D, Wadden T, Townsend R, et al. CPAP, weight loss, or both for obstructive sleep apnea. N Engl J Med. 2014; 370: 2265–2275.
- Friedman M, Salapatas A, Bonzelaar L. Updated Friedman staging system for obstructive sleep apnea. Adv Otorhinolaryngol. 2017; 80: 41–48.
- De Vito A, Carrasco Llatas M, Ravesloot M, Kotecha B, De Vries N, Hamans E, et al. European position paper on drug-induced sleep endoscopy: 2017 update. Clin Otolaryngol. 2018; 43: 1541–1552.
- Borowiecki B, Pollak C, Weitzman E, Rakoff S, Imperato J. Fibrooptic study of pharyngeal airway during sleep in patients with hypersomnia obstructive sleep-apnea syndrome. Laryngoscope. 1978; 88: 1310–1313.
- Croft C, Pringle M. Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci. 1991; 16: 504–509.
- Huntley C, Chou D, Doghramji K, Boon M. Preoperative drug induced sleep endoscopy improves the surgical approach to treatment of obstructive sleep apnea. Ann Otol Rhinol Laryngol. 2017; 126: 478–482.
- Aktas O, Erdur O, Cirik A, Kayhan F. The role of drug-induced sleep endoscopy in surgical planning for obstructive sleep apnea syndrome. Eur Arch Otorhinolaryngol. 2015; 272: 2039–2043.
- Blumen M, Latournerie V, Bequignon E, Guillere L, Chabolle F. Are the obstruction sites visualized on drug-induced sleep endoscopy reliable?. Sleep Breath. 2015; 19: 1021–1026.
- Faber J, Faber C, Faber A. Obstructive sleep apnea in adults. Dent Press J Orthod. 2019; 24: 99–109.
- Steffen A, Heiser C, Galetke W, Herkenrath S, Maurer J, Günther E, et al. Hypoglossal nerve stimulation for obstructive sleep apnea: updated position paper of the German Society of OtoRhino-Laryngology, Head and Neck Surgery. Eur Arch Otorhinolaryngol. 2022; 279: 61–66.
- Salamanca F, Leone F, Bianchi A, Bellotto R, Costantini F, Salvatori P. Surgical treatment of epiglottis collapse in obstructive sleep apnoea syndrome: epiglottis stiffening operation. Acta Otorhinolaryngol Ital. 2019; 39: 404–408.
- Valera F, Tamashiro E, de Araújo M, Sander H, Küpper D. Evaluation of the efficacy of supraglottoplasty in obstructive sleep apnea syndrome associated with severe laryngomalacia. Arch Otolaryngol Head Neck Surg. 2006; 132: 489–493.
- McNicholas W. The nose and OSA: variable nasal obstruction may be more important in pathophysiology than fixed obstruction. Eur Respir J. 2008; 32: 3–8.
- Gelardi M, Ciprandi G. The clinical importance of the nasal valve. Acta Biomed. 2019; 90: 31–33.
- Staevska M, Mandajieva M, Dimitrov V. Rhinitis and sleep apnea. Curr Allergy Asthma Rep. 2004; 4: 193–199.
- Mehrtash M, Bakker J, Ayas N. Predictors of continuous positive airway pressure adherence in patients with obstructive sleep apnea. Lung. 2019; 197: 115–121.
- Fujita S, Conway W, Zorick F, Roth T. Surgical correction of anatomic abnormalities in obstructive sleep apnea syndrome: uvulopalatopharyngoplasty. Otolaryngol Head Neck Surg. 1981; 89: 923–934.
- Rashwan M, Montevecchi F, Cammaroto G, Badr El Deen M, Iskander N, et al. Evolution of soft palate surgery techniques for obstructive sleep apnea patients: a comparative study for single-level palatal surgeries. Clin Otolaryngol. 2018; 43: 584–590.
- Pang K, Woodson B. Expansion sphincter pharyngoplasty: a new technique for the treatment of obstructive sleep apnea. Otolaryngol Head Neck Surg. 2007; 137: 110–114.
- Pinto J, Godoy L, Nunes H, Abdo K, Jahic G, Cavallini A, et al. Lateral-expansion pharyngoplasty: combined technique for the treatment of obstructive sleep apnea syndrome. Int Arch Otorhinolaryngol. 2020; 24: e107–e111.
- Nunes H, Vaz de Castro J, Favier V, Carsuzaa F, Kim M, Mira F, et al. Predictors of success of pharyngeal surgery in the treatment of obstructive sleep apnea: a narrative review. J Clin Med. 2023; 12: 6773.
- Vallianou K, Chaidas K. Surgical treatment options for epiglottic collapse in adult obstructive sleep apnoea: a systematic review. Life (Basel). 2022; 12: 1845.
- Masárová M, Formánek M, Jor O, Novák V, Vrtková A, Matoušek P, et al. Epiglottopexy is a treatment of choice for obstructive sleep apnea caused by a collapsing epiglottis. Life (Basel). 2022; 12: 1378.
- Torre C, Camacho M, Liu S, Huon L, Capasso R. Epiglottis collapse in adult obstructive sleep apnea: a systematic review. Laryngoscope. 2016; 126: 515–523.