Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 5
Open Access
Volume 5
Xu Bai Qiao, MD2; Jun Jiang, MD1; Jing Niu, MD1; Jingjing Lu3; Jike Lu, MD, PhD1*
*Corresponding Author: Jike Lu
Department of Orthopedic Surgery, Beijing United Family Hospital, Beijing, China.
Email: jike.lu@ufh.com.cn
Article Info
Received: Mar 03, 2025
Accepted: Mar 28, 2025
Published: Apr 04, 2025
Archived: www.jclinmedsurgery.com
Copyright: © Jike L (2025).
Abstract...
The Solitary Fibrous Tumor (SFT) is a rare soft tissue tumor with a substantially benign clinical presentation. However, a radiologically aggressive tumor mass was seen in 67-year-old male patient with a slow growing STF of the right lower leg who was noticed a swelling leg 6 years ago that was managed for symptoms relief of the varicose veins which was thought to cause his leg edema and swelling. In the recent 6 months, he felt his leg becoming bigger with pain and visited a vascular surgeon for varicose vein consultations, and then subsequently needle biopsy was performed for the leg mass and found STF. Radiological, histological and molecular findings are reported with discussion of diagnosis, surgical and postoperatively managements etc.
A review literature showed SFT’s clinical behavior as substantially benign, not surprisingly, aggressive or malignant neoplasms have been described. The potential risk of local recurrence and distant metastasis thus recommends wide surgical resection and careful long-term follow-up. Differential diagnosis may be quite complicated as SFT can mimic a variety of benign and malignant mesenchymal tumors. Immunohistochemically analysis for CD34, CD99, Vimentin and bcl-2 is definitely mandatory for confirming the diagnosis.
Keywords: Solitary fibrous tumor; Surgery; Immunohistogy; CD34 antigen; Aggressive; Metastasis; Recurrence.
Citation: Xu Bai Q, Jun J, Jing N, Jingling L, Jike L. Misdiagnosed a Locally Aggressive Solitary Fibrous Tumor of Lower Leg: A Case Study and Literature Review. J Clin Med Surgery. 2025; 5(1): 1190.
Introduction
Solitary Fibrous Tumor (SFT) is a rare mesenchymal, ubiquitous tumor, with an incidence of 1 per million per year. In the 2020 WHO classification [1], risk stratification models were recommended as a better mode to determine prognosis in SFT rather than malignant or not. The risk for metastasis is up to 35-45%, or even more, in series with a long-term follow-up [2].
SFT is considered a fibroblastic tumor with ubiquitous allocation affecting adult patients, usually from 20 to 70 years. In the largest series, the extra meningeal SFT cases were distributed as follows: abdominal cavity 31%, limbs 29%, pleura 22%, trunk 11% and others 7% (including head and neck) [2]. The median age reported in the largest series ranged from 50 to 60 years [2,3]. Clinically, SFTs present as a well-defined mass, which is more silent in primary pleural locations than extra-pleural primary sites.
Solitary fibrous tumor represents a spectrum of mesenchymal tumors, including tumors previously termed hemangiopericytoma that is classified as having intermediate biological potential (rarely metastasizing) in the 2002 World Health Organization classification system [1]. Primary solitary fibrous tumors in the extremities were not commonly occurring comparing with sites of occurrence in abdomen and pleura. Solitary fibrous tumors are categorized as intermediate biological potential with a low risk of metastasis and relatively indolent course under the 2002 WHO classification [1].
Tumors were scored for mitotic figures, cellularity, nuclear pleomorphism, and presence of necrosis. Mitotic index was calculated per 10 high-power fields, utilizing the highest count of 3-5 areas scored (depending on the number of available slides) [4]. The most cellular area of the tumor was scored for cellularity on a 3-point scale from 1=low (tumor predominately composed of sclerotic collagen bands with scattered, compressed spindle cells) to 2=moderate (many areas of increased cellularity with cells adjacent to one another) to 3=high (hypercellular tumor, with areas of nuclear overlap). Pleomorphism was scored on a 3-point scale from 1=low (cells monomorphic, with uniform nuclear features) to 2=moderate (increased nuclear pleomorphism, more prominent nucleoli, and rare multinucleated cells) to 3=high (hyperchromatic nuclei present with foci of marked pleomorphism and bizarre cells). Areas of abrupt change from classic solitary fibrous tumor morphology to diffuse high-grade sarcoma were regarded as poorly differentiated. Necrosis hemorrhage was scored as minimal (<10%) or positive (>10%), based on available histological sections.
However, the clinical behavior of individual tumors is notoriously difficult to predict. Furthermore, criteria for malignancy have not been consistent between published cases, and the historical attempts at the division of hemangiopericytoma and solitary fibrous tumor has prevented investigations into this class of tumors as a unified spectrum or entity [5-12]. Several histopathological criteria have been reported to be useful for determining malignancy in solitary fibrous tumor. These include increased tumor size, mitotic count, cellularity, presence of hemorrhage/necrosis, nuclear pleomorphism [5,11,9-15], and presence of sharply demarcated anaplastic/poorly differentiated foci (also regarded by some as ‘dedifferentiation’) [15]. Few immunohistochemically and no molecular markers are known to have prognostic significance. Not many studies had evaluated histopathological and clinic pathological SFT presentations.
Solitary Fibrous Tumor (SFT) is an uncommon neoplasm as arising from the pleura, intrathoracic organs as well as extra thoracic regions, including soft tissue. Symptoms of extra pleural SFT are non-specific (painless, non-tender, smooth, slow-growing mass) and related to the presence of a mass in deep soft tissue [16].
SFT is currently classified as a biologically “borderline” neoplasm, which means that the lesion may recur locally and almost never metastasize. To date only few cases of SFT arising from the extremities have been reported in the English literature [18,19].
The present study describes a patient with a slow growing tumor of the lower leg that was missed as a varicose vein swelling for last 6 years. Radiological, histological and immunohistochemically findings are discussed along with differential diagnosis, surgical treatment and short-term outcomes (six months postoperatively follow up).
Case description
A 67-year-old male with a long time history lower limb of varicose veins accompanied with chronic swelling around ankle, especially on the right leg which was diagnosed as drainage defect caused by varicose vein that led to leg swelling especially distal to the knee (Figure 1) and edema around right rankle, and was managed symptomatically. However, his upper lateral leg swelling was worsening last a year with distension feelings and pain sometimes. He was visited a vascular surgeon for his varicose vein but found a large mass over upper anterior lateral lower leg, originating from proximal anterior lateral tibia extending distally above the ankle joint between tibia and fibula. On physical examination, the mass was in size of 25.0 cm × 15.0 cm × 10.0 cm that was located in anterior lateral compartment of the lower leg (Figure 1). There was mild tenderness but not movable on palpation, no pulsation and no skin color alterations except visible varicose veins.
Preoperatively he had local and systemic staging. Preoperatively plain radiographs were taken based on distal lower leg edema that did not include proximal tibia and knee joint, therefore, no abnormalities were detected (Figure 2). Radiologically, tumors were considerably vascular, showing a moderate contrast enhancement in CT scans (Figure 3). Heterogeneity after contrast injection was not seen in our case. CT exhibits intermediate to high attenuation on unenhanced CT scans, and this heterogeneous attenuation was noticed. Low attenuation on unenhanced CT scans was present as geographic, focal or linear disposition and was observed (Figure 3). These low attenuated areas correspond with gross calcifications, necrosis, hemorrhage or cystic changes. In MRI, SFT appears as isointense in T1 weighted images and variable in T2 (Figures 4 & 5). Low intensity areas on T1 or T2 weighted images are due to calcifications, or collagen content and low cellularity. Moderate to strong enhancement with gadolinium is usually seen as it is consistent with vascular tumors.
The MRI features were highly suspicious for an undefined aggressive tumor such as fibrosarcoma or liposarcoma of soft tissue and a percutaneous needle biopsy was performed that showed Solitary Fibrous Tumor (SFT).
He had past medical history of hypertension, abnormal ECG, type 2 DM, Hyperlipidemia, dry eyes syndrome, and bilateral lower leg varicose vein diseases.
After MDT consultations with musculoskeletal oncologists, radiologists and tumor specialists, a wide local excision in the anterior and anterolateral compartments of the left leg was planned.
Operation procedures as follows: The patient was under general anesthesia, supine on operation table with above knee tourniquet without exsanguination. Routinely preparation and drapes of skin for whole leg were done. Skin incision from anterolateral proximal tibia just below lateral tibial plateau extended distally in anterolateral lower leg just above the ankle joint. Full thickness skin flap was made, meticulously dissection of the mass from proximal to distal including tumor mass penetrated to posterior compartment via interosseous membrane hole in upper part leg (Figure 1B). Dissection carefully to keep anterolateral and anterior compartment muscle intact, split muscles, if necessary, in line with muscle fiber alignment. The muscle atrophy was noticed. A careful dissection of the tumor from the anterior tibialis and the extensor digitorum muscle superficially and deeply from the extensor hallucis longus was performed. The deep branch of the common peroneal nerve and the anterior tibialis artery and vein were carefully dissected and protected. A meticulously dissection capsulated soft tissue tumor and excision of the neoplasm en bloc including extension through interosseous membrane between tibia and fibula in proximal 1/3 of the leg to posterior compartment of the leg and all tumors were completely excised (Figure 6). There was tumor invasion in proximal tibial bone, multiple focused lesions which were curettaged and burred with a high-speed burr. After excision all invasive tumor in tibia the cavity was washed thoroughly and filled with cement (Figure 7). Meticulously hemostasis was done. The procedure was carried out without complications and the pathologic findings and immunohistological studies confirmed the SFT diagnosis and revealed tumor free margins on all specimens. The leg was immediately smaller after surgery (Figure 1B), and maintained normal function of the ankle foot toes.
According to the pathologic findings and immunohistochemically findings, a diagnosis of low grade of solitary fibrous tumor was made.
Microscopically, histological and pathological photos of the tumor consisted of spindle cells arranged in fascicles, with interposed thick bands of collagen (Figure 8). The tumor was richly vascularized and contained areas with dilated vessels. Capillary proliferation was prominent. Cellular atypia was unremarkable. Mitotic figures were rare. No necrosis, hemorrhage or vascular invasion was present. Immunohistochemically studies showed that the tumor cells exhibited strong immunoreactivity for CD34 and bcl-2. The tumor cells were negative for Epithelial Membrane Antigen (EMA), smooth muscle actine and S100 protein (Figure 9).
He was discharged home 5 days after surgery allowed weight bearing as tolerated with a walking aide, and referred him for oncologist review for further managements to prevent recurrence. However, 6 months postoperatively follow-up, he had no adjuvant chemotherapy or radiotherapy administered by oncologists based on surgical clearance and low grade of the tumor. The radiographs and, 6 months after surgery, did not reveal any recurrence (Figure 10). The photographs showed the leg is kept in almost in normal shape (Figure 11).

Figure 1: Preoperatively photographs showed a large mass over anterolateral proximal tibia (arrows in A and C); Postoperatively, the mass was clearly disappeared and leg was thinner (B).

Figure 2: Preoperative radiographs were taken but did not include proximal tibia due to physician was not considered lesions in proximal lower leg because of distal leg and ankle edema, therefor no abnormalities either in bones or soft tissues were seen in AP and lateral views (A & B).
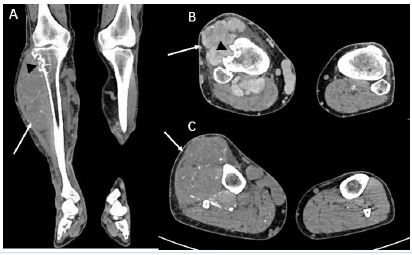
Figure 3(1): CT scans of the coronal and axial views showed large soft tissue mass in anterolateral compartment of the lower leg (arrows in A-C); bone erosions seen in proximal lateral tibia (arrow head in A and B with moderate enhancement on enhanced CT).
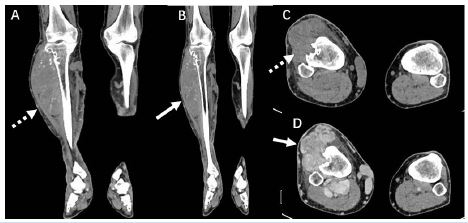
Figure 3(2): Preoperative CT studies showed tumor mass in proximal anterior lateral compartment of the lower leg (A and C non contrast images, dashed arrows) (B and D contrast enhanced mildly and moderately enhanced images (arrows).
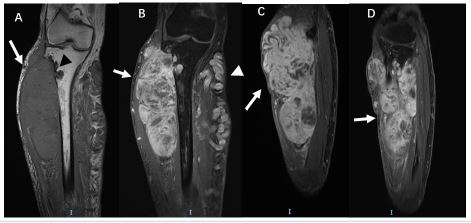
Figure 4(1): (A) MRI T-1 weighted MRI coronal view showing large soft tissue mass (a white arrow) and proximal lateral tibia bone scalloping erosions (a black arrow head); (B, C and D) T-1 test sequence showing large soft tissue mass, multi-lobulated with low signals in substance of the mass (calcifications), seems to be capsulated with septum (arrows in B, C and D); An white arrow head indicated varicose vein over medial aspect of the tibia in B.
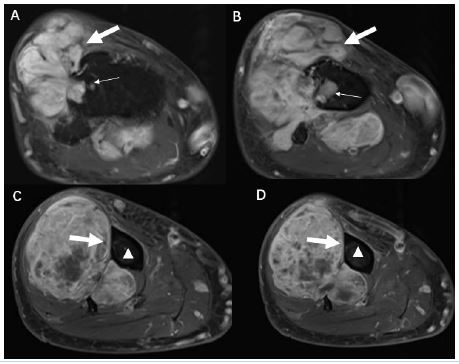
Figure 4(2): Axial views of T1 TSE sequence showing large soft tissue mass, multi-lobulated (arrows in A and B) with low signals in substance of the mass (calcifications in B, C and D), and the tumors extending to posterior compartment of the leg (A and B, arrows); bone erosions seem to be caused by pressure in proximal lateral tibia (thin white arrows) where the volume of the tumor mass is bigger but distally the tibial bone has no erosions at all (white triangles).
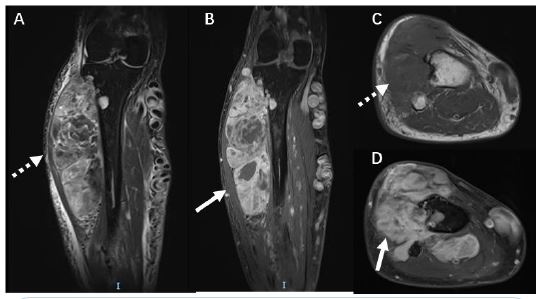
Figure 5(1): MRI T-1 TSE sequence showed tumor mass was moderately enhanced in contrast MRI study (B and D arrows); A & C MRI images showed tumor mass in non-enhanced conditions (dashed arrows).
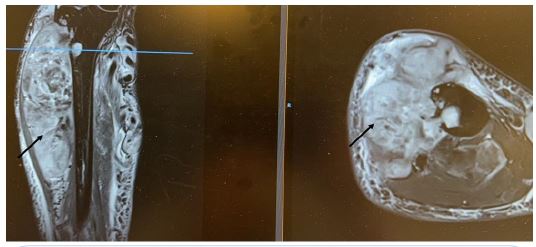
Figure 5(2): MRI T-2 weighted enhanced coronal and axial views showing moderate enhancement in the tumor mass (arrows).
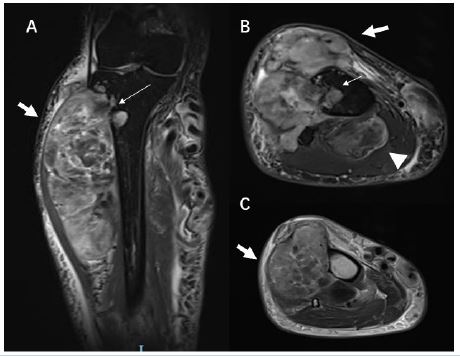
Figure 5(3): MRI T-2 TSE sequence showing large soft tissue mass sitting in proximal and middle anterior lateral compartment of the leg (arrows in A-C), bone erosions seen in proximal lateral tibia (thin arrows) and the tumor extending to posterior compartment of the leg (an arrow head in B).
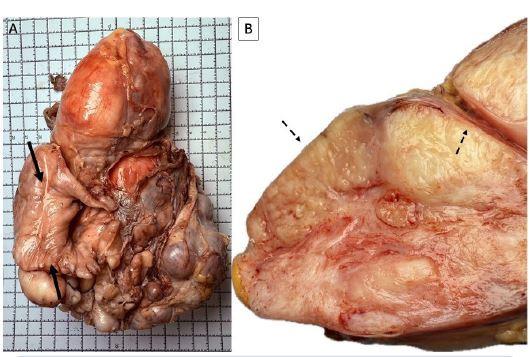
Figure 6: Gross specimen of the tumor mass after fixation from Formalin, the longest distance was 19 cm, most of the tumor from anterior anterolateral compartment of the lower leg but a kidney size tumor extending posterior compartment of the leg was taken out en bloc as well (an arrow in A); Cross-sectional specimen showed a multilobulated yellowish capsulated with septums (B dashed arrows).
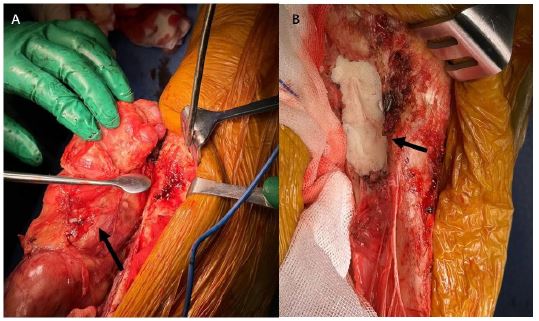
Figure 7(1): Due to slow growing history of the tumor approximately 25.0 cm × 15.0 cm × 10.0 cm displacing all muscles of the anterior compartment of the leg. A large tumor mass was excised en bloc (an arrow); bone lesions were curettaged and the void was filled with cement (an arrow).
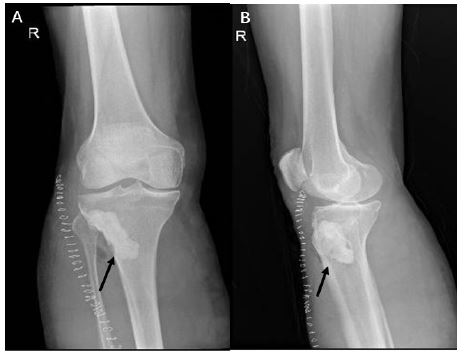
Figure 7(2): Postoperative radiographs showed bone erosion upper lateral tibia was curettaged completely and cement to fill the void completely (arrows in A and B).
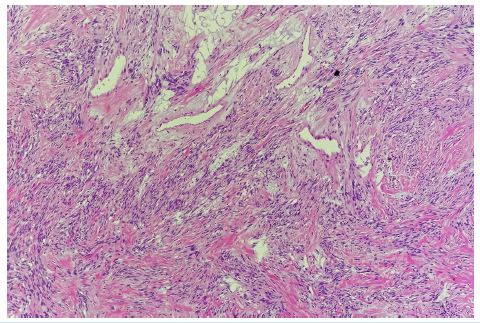
Figure 8: The tumor consisted of spindle cells arranged in fascicles, with interposed thick bands of collagen.
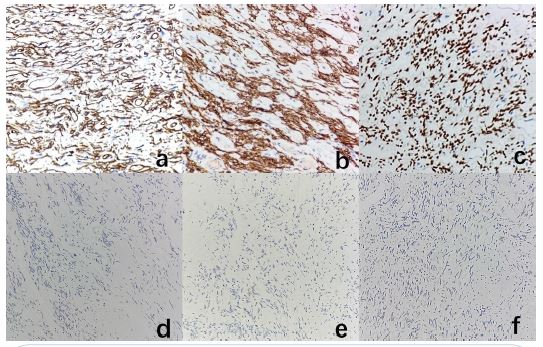
Figure 9: The tumor cells exhibited strong positive immunoreactivity for CD34 (A), BCl-2 (B) and STAT6 (C); Negative for EMA (D), SMA (E) and S-100 protein (F).
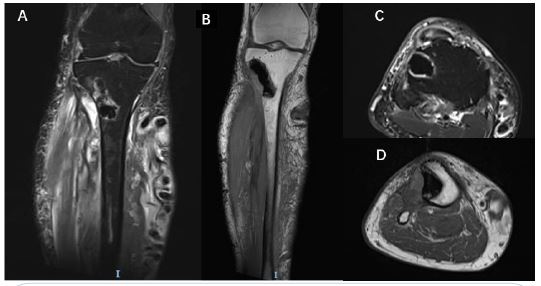
Figure 10: 6 months postoperatively follow-up MRI in T-1 (A and C) and T-2 (B and D) showed that no recurrent lesions or tumors in any compartment of the leg except mild edema at intermuscular spaces.

Figure 11: Six months postoperatively photographs showed tumor site (arrows in A and B) in normal shape compared with contralateral side in B. Varicose veins are seen in bilateral legs especially distal lower legs.
Discussion
For decades Solitary Fibrous Tumor has been in debate as to whether the tumor originated from mesothelial or mesenchymal cells. Actually, on the basis of immunohistochemically finding CD34 positivity, most authors believe that this tumor arises from pluripotential mesenchymal cells located in the connective tissue [20,21]. A huge variety of extra pleural locations, such as the thyroid gland, salivary glands, upper respiratory tract, liver, epicardium, kidney, mediastinum, orbit, meninges, periosteum, adrenal gland, scrotum, spinal cord and soft tissues, has been described [20,21].
Nowadays the diagnosis of these tumors remains problematic if just based on histology. Radiologically, tumors are considerably vascular, showing moderate to strong contrast enhancement in 65% of cases in CT scans and, interestingly, in 35% of cases large collateral feeding vessels were verified [22]. Heterogeneity after contrast injection was more frequently seen in 76.5% more aggressive and 40.0% more indolent SFTs [23]. SFT exhibits intermediate to high attenuation on unenhanced CT scans, reflecting a high density of collagen fibers along with a rich capillary network [24]. In other series, heterogeneous attenuation was detected in 88% of cases. Low attenuation on unenhanced CT scans could be present as geographic, focal or linear disposition and is observed in up to 86%. These low attenuated areas correspond with gross necrosis, hemorrhage or cystic changes. In MRI, SFT appears as isointense in T1 weighted images and variable in T2. Low intensity areas on T1 or T2 weighted images are due to collagen content and low cellularity. Strong enhancement with gadolinium is usually seen as it is consistent with vascular tumors [25-31].
The 18F-FDG PET has not been shown to be a determinant in distinguishing indolent SFT from aggressive SFT in a series of 17 patients with confirmed SFT diagnosis [26,31]. Obviously, different metabolic activity could be detected in some cases [25,26], especially if dedifferentiated SFT is considered. However, it is unclear if mild overproduction of insulin-like growth factor II could have some influence on the PET scan.
Microscopically, SFTs are well circumscribed and characterized by the proliferation of capillaries surrounded by masses of round or spindle shaped cells without an obvious pattern [34]. A combination of growth patterns is typically present, including herringbone, neural with wavy nuclei, storiform or a characteristic arborizing vascular pattern described as hemangiopericytic [35]. Significantly increased cellularity, nuclear atypia, mitotic activity (>4 mitoses/10 HPF) and areas of necrosis should be considered as malignancy criteria, and are associated with an aggressive clinical behavior [36].
The so-called “patternless pattern” may mimic other tumors, thus the differential diagnosis is always extensive, requiring an immunohistochemically analysis for CD34, vimentin and CD99 [37]. CD34 antigen, a transmembrane glycoprotein, being a helpful modality to diagnose solitary fibrous tumors [38] because it is strongly positive in most cases of SFT and as our case is positive as well. The tumor is generally labeled uniformly for vimentin, an intermediate filament protein expressed in all mesenchymal cells. Expression of vimentin is also detected in some lymphomas, sarcomas and melanoma. Bcl-2 protein has also been proposed to be a helpful marker to diagnose solitary fibrous tumor [38,39]. Other useful immunohistochemically markers for differential diagnosis are CD-99, smooth muscle actine (detected in benign and malignant smooth muscle tumors), S100 protein (detected in peripheral nerve sheath, cartilage tumors and melanoma) and cytocheratins [40,41]. Given the wide range of morphology, SFT can potentially be mistaken for other benign and malignant soft tissue tumors, but the main diagnostic pitfall includes hemangioperycitoma, monophasic synovial sarcoma and malignant fibrous histiocytoma.
The morphologic distinction with hemangioperycitoma can be rather difficult to be made. However, demonstration of areas within the same tumor showing some other morphologic patterns, such as storiform or herringbone pattern, should be useful in the diagnosis of SFT. SFT may also be misdiagnosed as a malignant fibrous histiocytoma. However, the lack of a diffused cytologic atypia, a low mitotic activity, and the absence of necrosis, however, will be useful to rule out malignant fibrous histiocytoma in most cases. The monophasic synovial sarcoma should be excluded as well, due to an overall pattern which is generally uniformly cellular and to immunohistochemically analysis focally positive with keratin antibodies [42-44] and Epithelial Membrane Antigen (EMA).
Benign and malignant fibrous histiocytoma, fibrosarcoma and desmoids tumor do not show immunoreactivity to CD34 antibody. Neurofibroma and malignant peripheral nerve sheath tumors can show variable staining for CD34 and bcl-2, SFTs show a more intense reactivity for both markers [38]. In a large amount of these tumors, immunoreactivity for S100 protein may be of aid in the differential diagnosis.
Because of the rarity of this tumor, little is known about its clinical behavior. Vallat-Decouveleare et al [14,36] & Gold et al [45] found local recurrence ranging from 4.3% to 6.7% and metastases from 5.4% to 5.3%, respectively. Sites of distant metastases were lung, liver, bones, mesentery, mediastinum and retro-peritoneum. Factors suggesting malignancy indicated by Vallat-Decouveleare et al. [14,36] were malignant histologic features, such as markedly increased cellularity, nuclear atypia, mitotic activity (>4 mitoses/10 HPF) and areas of necrosis. Gold et al [13,44], also found that tumors greater than 10 cm had a statistically significant worse outcome for metastases. Noteworthily, in our case report, the pathologic findings of a tumor with low malignant potential contrasted with its clinical behavior. The choice for a conservative treatment was difficult and debated. The rapid growth of the tumor was highly suspected for an aggressive lesion but, as confirmed by our follow-up, the clinical behavior was finally benign. Our patient, in fact, has just completed his first year without any signs of focal or distant disease.
Contrary to what was initially thought, SFT is sensitive to Radiotherapies (RT). Interestingly, a retrospective series of 40 patients treated with definitive RT (60 Gy) reported an Overall Response Rate (ORR) of 67% with 5-year local control of 81.3% [46]. Therefore, SFT cases at the limit of resectability, or those cases in which a marginal resection is done, especially those cases with a high mitotic rate, could benefit from neoadjuvant RT. Furthermore, the scheme of trabectedin plus low dose RT seems very active in several STS subtypes [47], and could also be an alternative in cases requiring tumor shrinkage in order to facilitate limb sparing surgery, for instance. In any case, every treatment decision should be taken by a multidisciplinary consultation.
Chemotherapy has typically been used in the advanced or metastatic setting of SFT patients. However, very limited prospective evidence on the activity of standard cytotoxic drugs has been available in SFT, and furthermore, no specific clinical trials addressing the value of chemotherapy have been reported on SFT. Some of these series provided potential useful information regarding the different SFT subtypes included in the former 2013 STS classification of the WHO (typical, malignant and dedifferentiated subtypes) [48]. Conversely, in terms of the value of cytotoxic drugs in those SFTs exhibiting less aggressive features, the formerly defined typical and malignant SFT, chemotherapy efficacy remains controversial.
In non-dedifferentiated SFT, antiangiogenic agents are more active, by indirect comparison, than chemotherapy. Pazopanib is the recommendation as first line [47], based on its least toxicity profile and the efficacy derived from a phase II trial. Further, the survival length seems superior compared with the historical use of chemotherapy. Other antiangiogenics, such as sunitinib [49,50] or axitinib, have demonstrated positive activity in SFT and could be used sequentially. Regarding the use of doxorubicin-based regimens in non-dedifferentiated SFT, it is detrimental to the antiangiogenic therapy [51] which can be used in the context of antiangiogenic refractory SFT, especially dacarbazine-based chemotherapy. Trabectedin could also be an option to consider for the treatment of progressing SFT [52,53].
Conclusion
On the whole, SFT has a benign clinical course, but the clinical behavior is unpredictable and the relationship between morphology and clinical behavior is poor. Complete surgical resection is commonly accepted as a treatment of choice for limb SFT. A close long-term follow-up has to be recommended even after radical excision.
References
- WHO. Classification of Tumors Editorial Board. Soft Tissue and Bone Tumours. In WHO Classification of Tumors Series, 5th ed.; International Agency for Research on Cancer: Lyon, France. 2020: 3.
- Demicco EG, Park MS, Araujo DM, Fox PS, Bassett RL, Pollock RE, et al. Solitary fibrous tumor: A clinic pathological study of 110 cases and proposed risk assessment model. Mod Pathol. 2012; 25: 1298–1306.
- Salas S, Resseguier N, Blay JY, et al. Prediction of local and metastatic recurrence in solitary fibrous tumor: Construction of a risk calculator in a multicenter cohort from the French Sarcoma Group (FSG) database. Ann Oncol. 2017; 28: 1979–1987.
- Trojani M, Contesso G, Coindre JM, et al. Soft-tissue sarcomas of adults; study of pathological prognostic variables and definition of a histopathological grading system. Int J Cancer. 1984; 33: 37–42.
- England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol. 1989; 13: 640–658.
- Enzinger FM, Smith BH. Hemangiopericytoma. An analysis of 106 cases. Hum Pathol. 1976; 7: 61–82.
- Fisher JH. Hemangiopericytoma: a review of twenty cases. Can Med Assoc J. 1960; 83: 1136–1139.
- Goldman SM, Davidson AJ, Neal J. Retroperitoneal and pelvic hemangiopericytomas: clinical, radiologic, and pathologic correlation. Radiology. 1988; 168: 13–17.
- Insabato L, Siano M, Somma A, et al. Extrapleural solitary fibrous tumor: a clinicopathologic study of 19 cases. Int J Surg Pathol. 2009; 17: 250–254.
- Nielsen GP, O’Connell JX, Dickersin GR, et al. Solitary fibrous tumor of soft tissue: a report of 15 cases, including 5 malignant examples with light microscopic, immunohistochemically, and ultrastructural data. Mod Pathol. 1997; 10: 1028–1037.
- Robinson LA. Solitary fibrous tumor of the pleura. Cancer Control. 2006; 13: 264–269.
- Espat NJ, Lewis JJ, Leung D, et al. Conventional hemangiopericytoma: modern analysis of outcome. Cancer. 2002; 95: 1746–1751.
- Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002; 94: 1057–1068.
- Vallat-Decouvelaere AV, Dry SM, Fletcher CD. Atypical and malignant solitary fibrous tumors in extrathoracic locations: evidence of their comparability to intra-thoracic tumors. Am J Surg Pathol. 1998; 22: 1501–1511.
- Mosquera JM, Fletcher CD. Expanding the spectrum of malignant progression in solitary fibrous tumors: a study of 8 cases with a discrete anaplastic component—is this dedifferentiated SFT?. Am J Surg Pathol. 2009; 33: 1314–1321.
- Anders JO, Aurich M, Lang T, Wagner A. Solitary fibrous tumor in the thigh: review of the literature. J Cancer Res Clin Oncol. 2006; 132: 69–75.
- Salas S, Resseguier N, Blay JY, et al. Prediction of local and metastatic recurrence in solitary fibrous tumor: Construction of a risk calculator in a multicenter cohort from the French Sarcoma Group (FSG) database. Ann Oncol. 2017; 28: 1979–1987.
- Abe S, Imamura T, Tateishi A, Park P, Nakano H, Harasawa A. Intramuscular solitary fibrous tumor: a clinic pathological case study. J Comp Assist Tomogr. 1999; 23: 458–462.
- Gengler C, Guillou L. Solitary fibrous tumour and haemangiopericytoma: evolution of a concept. Histopathology. 2006; 48: 63–74.
- Wignall OJ, Moskovic EC, Thway K, Thomas JM. Solitary fibrous tumors of the soft tissues: review of the imaging and clinical features with histopathologic correlation. AJR Am J Roentgenol. 2010; 195: 55–62.
- Wignall OJ, Moskovic EC, Thway K, Thomas JM. Solitary fibrous tumors of the soft tissues: Review of the imaging and clinical features with histopathologic correlation. Am J Roentgenol. 2010; 195: W55–W62.
- Helage S, Revel MP, Chabi ML, Audureau E, Ferretti G, Laurent F, et al. Solitary fibrous tumor of the pleura: Can computed tomography features help predict malignancy? A series of 56 patients with histopathological correlates. Diagn Interv Imaging. 2016; 97: 347.
- Rosado-de-Christenson ML, Abbott GF, McAdams HP, Franks TJ, Galvin JR. From the archives of the AFIP: Localized fibrous tumor of the pleura. Radiographics. 2003; 23: 759–783.
- Ginat DT, Bokhari A, Bhatt S, Dogra V. Imaging features of solitary fibrous tumors. Am. J. Roentgenol. 2011; 196: 487–495.
- Tazeler Z, Tan G, Aslan A, Tan S. The utility of 18F-FDG PET/CT in solitary fibrous tumors of the pleura. Rev Esp Med Nucl Imagen Mol. 2016; 35: 165–170
- Wignall OJ, Moskovic EC, Thway K, Thomas JM. Solitary fibrous tumors of the soft tissues: Review of the imaging and clinical features with histopathologic correlation. Am J Roentgenol. 2010; 195: W55–W62.
- Helage S, Revel MP, Chabi ML, et al. Solitary fibrous tumor of the pleura: Can computed tomography features help predict malignancy? A series of 56 patients with histopathological correlates. Diagn Interv Imaging. 2016; 97: 347–353.
- Rosado-de-Christenson ML, Abbott GF, McAdams HP, Franks TJ, Galvin JR. From the archives of the AFIP: Localized fibrous tumor of the pleura. Radiographics. 2003; 23: 759–783.
- Ginat DT, Bokhari A, Bhatt S, Dogra V. Imaging features of solitary fibrous tumors. Am J Roentgenol. 2011; 196: 487–495.
- Tazeler Z, Tan G, Aslan A, Tan S. The utility of 18F-FDG PET/CT in solitary fibrous tumors of the pleura. Rev Esp Med Nucl Imagen Mol. 2016; 35: 165–170.
- Ramdial PK, Madaree A. Aggressive CD34-positive fibrous scalp lesion of childhood: extrapulmonary solitary fibrous tumor. Pediatr Dev Pathol. 2001; 4: 267–275.
- Schellini SA, Hoyama E, Marques ME, Abreu ES, Yamashita S. Orbital solitary fibrous tumor: report of two cases and literature review. Jpn J Ophthalmol. 2003; 47: 415–418.
- Daigeler A, Lehnhardt M, Langer S, Steinstraesser L, Steinau HU, Mentzel T. Clinicopathological findings in a case series of extrathoracic solitary fibrous tumors of soft tissues. BMC Surg. 2006; 6: 10.
- Suster S, Nascimento AG, Miettinen M, Sickel JZ, Moran CA. Solitary fibrous tumors of soft tissue. A clinicopathologic and immunohistochemically study of 12 cases. Am J Surg Pathol. 1995; 19: 1257–1266.
- Vallat-Decouvelaere AV, Dry SM, Fletcher CD. Atypical and malignant solitary fibrous tumors in extrathoracic locations: evidence of their comparability to intra-thoracic tumors. Am J Surg Pathol. 1998; 22: 1501–1511.
- Clayton AC, Salomão DR, Keeney GL, Nascimento AG. Solitary fibrous tumor: a study of cytologic features of six cases diagnosed by fine-needle aspiration. Diagn Cytopathol. 2001; 25: 172–176.
- Akisue T, Matsumoto K, Kizaki T, Fujita I, Yamamoto T, Yoshiya S. Solitary fibrous tumor in the extremity: case report and review of the literature. Clin Orthopaed Rel Res. 2003; 411: 236–244.
- Hasegawa T, Matsuno Y, Shimoda T, Hasegawa F, Sano T, Hirohashi S. Extrathoracic solitary fibrous tumors: their histological variability and potentially aggressive behavior. Hum Pathol. 1999; 30: 1464–1473.
- Guerra MF, Amat CG, Campo FR, Pérez JS. Solitary fibrous tumor of the parotid gland: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94: 78–82.
- Bauer JL, Miklos AZ, Thompson LD. Parotid gland solitary fibrous tumor: a case report and clinicopathologic review of 22 cases from the literature. Head Neck Pathol. 2011.
- Chilosi M, Facchetti F, Tos APD, Lestani M, Morassi ML, Martignoni G. bcl-2 expression in pleural and extra pleural solitary fibrous tumours. J Pathol. 1997; 181: 362–367.
- England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol. 1989; 13: 640–658.
- Van de Rijn M, Lombard CM, Rouse RV. Expression of CD34 by solitary fibrous tumors of the pleura, mediastinum, and lung. Am J Surg Pathol. 1994; 18: 814–820.
- Gold JS, Antonescu CR, Hajdu C, Ferrone CR, Hussain M, Lewis JJ. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002; 94: 1057–1068.
- Haas RL, Walgreen I, Lecointe-Artzner E, et al. Radiation Therapy as Sole Management for Solitary Fibrous Tumors (SFT): A Retrospective Study from the Global SFT Initiative in Collaboration with the Sarcoma Patients EuroNet. Int J Radiat Oncol Biol Phys. 2018; 101: 1226–1233.
- Martin-Broto J, Hindi N, Lopez-Pousa A, et al. Assessment of Safety and Efficacy of Combined Trabectedin and Low-Dose Radiotherapy for Patients with Metastatic Soft-Tissue Sarcomas: A Nonrandomized Phase 1/2 Clinical Trial. JAMA Oncol. 2020; 6: 535–541.
- Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F. WHO Classification of Tumors of Soft Tissue and Bone, 4th ed.; IARC Press: Lyon, France. 2013: 5.
- Maruzzo M, Martin-Liberal J, Messiou C, Miah A, Thway K, Alvarado R, et al. Pazopanib as first line treatment for solitary fibrous tumours: The Royal Marsden Hospital experience. Clin. Sarcoma Res. 2015; 5: 5.
- Mulamalla K, Truskinovsky AM, Dudek AZ. Rare case of hemangiopericytoma responds to sunitinib. Transl. Res. 2008; 151: 129–13.
- George S, Merriam P, Maki RG, Van den Abbeele AD, Yap JT, Akhurst T, et al. Multicenter phase II trial of sunitinib in the treatment of nongastrointestinal stromal tumor sarcomas. J Clin Oncol. 2009; 27: 3154–3160.
- Domont J, Massard C, Lassau N, Armand JP, Le Cesne A, Soria JC. Hemangiopericytoma and antiangiogenic therapy: Clinical benefit of antiangiogenic therapy (sorafenib and sunitinib) in relapsed malignant haemangioperyctoma /solitary fibrous tumour. Investig. New Drugs. 2010; 28: 199–202.
- Martin-Broto J, Hindi N, Grignani G, Martinez-Trufero J, Redondo A, Valverde C, et al. Nivolumab and sunitinib combination in advanced soft tissue sarcomas: A multicenter, single-arm, phase Ib/II trial. J. Immunother. Cancer. 2020: 8.
- Valentin T, Fournier C, Penel N, et al. Sorafenib in patients with progressive malignant solitary fibrous tumors: A subgroup analysis from a phase II study of the French Sarcoma Group (GSF/GETO). Investig. New Drugs. 2013; 31: 1626–1627.