Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 5
Open Access
Volume 5
*Corresponding Author: Kimiyasu Yoneyama
Department of Breast Surgery, Hiratsuka City Hospital, Hiratsuka, Japan.
Email: key13213@yahoo.co.jp
Article Info
Received: Feb 20, 2025
Accepted: Mar 13, 2025
Published: Mar 20, 2025
Archived: www.jclinmedsurgery.com
Copyright: © Yoneyama K (2025).
Abstract...
Introduction and importance: Breast cancer can grow in a variety of ways, but pedunculated growth is extremely rare. We report a case of breast cancer that showed pedunculated growth outside the breast.
Case presentation: A 76-year-old woman visited our hospital complaining of a pedunculated mass on her left breast that had been present for several years. A pedunculated mass measuring 10 cm in diameter was found on the cephalad side of the nipple in the left breast. There was no ulceration on the skin surface, and no abnormality was found in the nipple. Contrast-enhanced CT showed the mass to be non-uniformly enhancing internally with left axillary lymph node enlargement. Although no preoperative tissue diagnosis was obtained, a left partial mastectomy and axillary lymph node dissection were performed based on a clinical diagnosis of left breast cancer.
Clinical discussion: Histopathological findings showed infiltration and proliferation of atypical cells in a fused glandular duct-like pattern, consistent with adenocarcinoma. Metastasis was found in the axillary lymph node specimen. The tumor was hormone receptor-negative and HER2-negative. The patient was followed up without postoperative chemotherapy or radiotherapy.
Conclusion: We encountered a rare case of breast cancer that showed pedunculated extramammary growth. This case is reported because of its unique growth pattern and interesting histological findings.
Keywords: Breast tumor; Breast cancer; Pedunculated tumor.
Citation: Yoneyama K. A Case of Breast Cancer Showing a Pedunculated Growth Pattern. J Clin Med Surgery. 2025; 5(1): 1188.
Introduction
Breast cancer is one of the most common cancers affecting women and can develop in various ways. Initially, the tumor remains within the breast, but as it progresses, it can protrude from the skin surface. In many cases, ulcers form on the skin surface, accompanied by discharge of exudate, bleeding, and necrosis. However, pedunculated growth covered by the epidermis is extremely rare. This report describes a case of breast cancer that showed pedunculated growth outside the breast and was written in accordance with the SCARE criteria [1].
Presentation of case
A 76-year-old woman visited our hospital complaining of a pedunculated mass on the upper left breast that had been present for several years. The mass was painless and had been gradually enlarging for at least a year. There was no family history of breast cancer or BRCA abnormality. Palpation revealed a mass measuring 10 cm in diameter on the cephalad side of the nipple on the left breast (Figures 1a & 1b). The surface of the tumor was covered with slightly reddish skin, but there was no ulceration. It was connected to the left breast by normal skin. No abnormality was found in the nipple itself.
Mammography revealed a high-density mass protruding from the left breast (Figure 2). Ultrasound examination revealed a mass with an uneven internal echo signal (Figure 3a). Blood flow was also observed inside the tumor (Figure 3b). Contrast-enhanced computed tomography revealed a mass with uneven internal contrast (Figure 4) and left axillary lymph node enlargement.
Breast cancer was suspected, so a left partial mastectomy, including the bottom attachment of the pedicle, and a sentinel lymph node biopsy were performed. Intraoperative rapid pathology revealed left axillary lymph node metastasis of adenocarcinoma, and left axillary lymph node dissection was performed (Figure 5).
Examination of the resected specimen showed a white-to-red mass with a clear border visible to the naked eye (Figure 6). Histologically, atypical cells were seen to infiltrate and proliferate in a fused glandular tubular, simple glandular tubular, trabecular, and solid pattern. These findings were consistent with adenocarcinoma (Figure 7). The tumor cells were CK7-positive, estrogen receptor-negative, progesterone receptor-negative, and HER2-negative. MIB-1 expression was 20%.
At the patient’s request, no postoperative chemotherapy or radiotherapy was administered. As of 1 year after surgery, follow-up observation has not revealed any signs of recurrence or metastasis, including locally.

Figure 1: Clinical photographs showing a 10 cm diameter mass cephalad to the nipple on the left breast. (A) The tumor was covered with reddish skin, and no ulceration was observed.
(B) There was no apparent abnormality in the nipple.
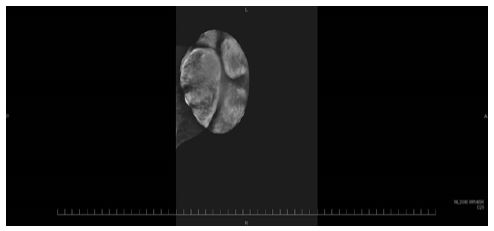
Figure 2: Mammogram showing a high-density mass protruding from the breast.
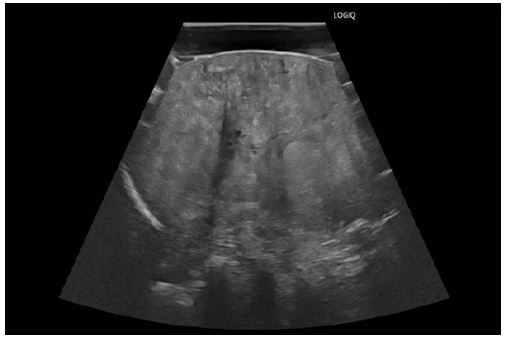
Figure 3: Findings on ultrasound examination. (A) A mass with an uneven internal echo signal. (B) Blood flow was observed inside the tumor.
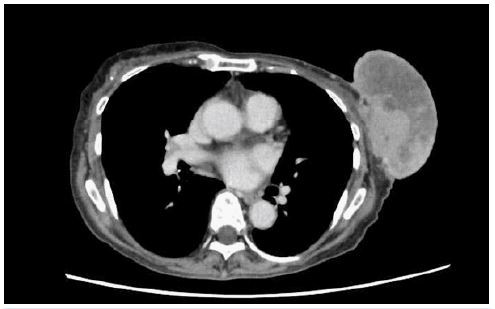
Figure 4: Contrast-enhanced computed tomography showing a mass with uneven internal contrast. Infiltration into the breast was suspected.

Figure 5: Clinical photograph obtained after left partial mastectomy. The area of the breast resection was extensive because the base of the pedicle was also removed.
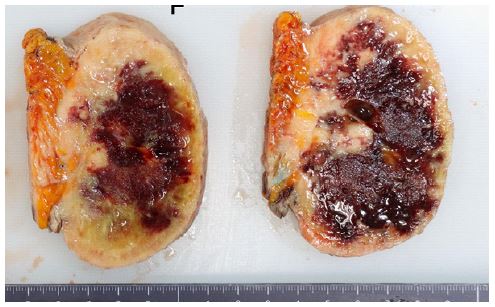
Figure 6: Macroscopic examination showed that the tumor was white-to-red with a clear border.
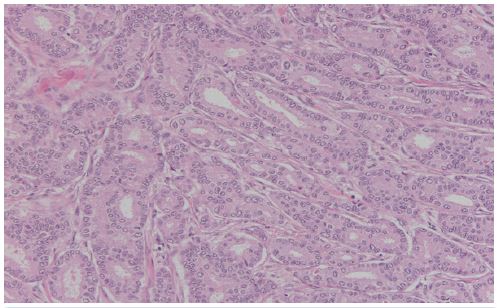
Figure 7: Histological examination revealed proliferation of atypical cells in a fused glandular duct-like pattern, consistent with adenocarcinoma.
Discussion
Breast cancer shows various growth patterns as it progresses. In many cases, an untreated tumor eventually becomes exposed on the skin surface and forms an ulcer, leading to bleeding and exudation. Some tumors protrude and rise above the skin surface without ulceration of the skin surface. In our case, there was no bleeding or exudation and the surface of the tumor was dry. There have been few reports of breast cancer that shows a pedunculated growth pattern, whereby the tumor protrudes outside the breast and is connected to the breast tissue by normal skin, as in our patient.
In view of the external morphology, differentiation from skin tumors is important. The first skin tumor to exclude is pedunculated basal cell carcinoma, but there have been few reports on this tumor [2,3]. Although these tumors can develop anywhere on the body, true basal cell carcinoma is more likely to develop on the face whereas pedunculated basal cell carcinoma is more likely to develop on the trunk. Furthermore, there have been no reports of such tumors being as large as the one in our case. Moreover, the surface of a pedunculated basal cell carcinoma is predominantly black, which makes it possible to differentiate it. However, some cases have an appearance similar to that in this case, so caution is required [4].
The tumors with most similarity in external morphology is fibroepithelial stromal polyps and soft fibromas. Fibroepithelial stromal polyps are benign tumors found in the skin, oral cavity, urinary tract, and genitals but are rarely found in the nipple. Soft fibromas can also occur anywhere in the body, but when they occur in the breast, they are often reported to originate from the nipple [5-9]. There are very few cases in which they originate from skin other than the nipple [10]. Some tumors are large, as in our patient, and the skin appearance is similar, so it may be difficult to differentiate based on external morphology alone.
A comprehensive diagnostic process that includes imaging is necessary. In this case, contrast computed tomography showed axillary lymph node enlargement, which was suggestive of malignancy. Therefore, the tumor was judged to be malignant. However, the axillary lymph node enlargement could have been reactive, and in retrospect, we believe that making a definitive diagnosis by needle biopsy before surgery would have been prudent.
There have also been reports of lipomas and lipomatous nevi that show pedunculated growth, but these are extremely rare [11,12]. In the case of lipoma, the tumor surface is completely covered by normal skin, making differentiation straightforward.
Treatment of a pedunculated breast cancer is no different from that of normal breast cancer, including surgery. However, it is important to note that the tumor is also present within the stalk, which is covered by normal skin. The tumor spreads into the breast via the stalk, so relatively wide resection of the breast is required. In our case, mastectomy was given careful consideration, but partial resection was performed at the patient’s request. Fortunately, postoperative pathology determined that the resection was complete. However, it would have been better to perform magnetic resonance imaging before surgery for more accurate assessment of the spread within the breast.
The histopathological findings in this case indicated adenocarcinoma that was estrogen receptor-negative, progesterone receptor-negative, HER2-negative, CK7-positive, and CK20-negative with MIB-1 expression of 20%. Despite its hormone receptor-negative status, the tumor was diagnosed as breast cancer, ductal type.
Conclusion
We have encountered a case of breast cancer that showed an extremely rare pedunculated extramammary growth pattern. This case is reported because of its unusual growth pattern and findings on histopathology.
Declarations
Ethical approval: Our institution does not require ethical approval for case reports that are deidentified and collected retrospectively.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Registration of research studies: This is a case report, and registration was required.
References
- Sohrabi C, Mathew G, Maria N, Kerwan A, Franchi T, Agha RA. The SCARE 2023 guideline: updating consensus Surgical Case Report (SCARE) guidelines. Int J Surg Lond Engl.
- Y Hanaoka, S Matsui, K Fukuyama. A case of pedunculated basal cell carcinoma of the abdomen. Clinical Dermatology. 2015; 69: 935-938.
- Y Yamamoto, S Miyagawa. A case of pedunculated basal cell carcinoma of the waist. 2006; 60: 611-613.
- M Kato, M Akahoshi, H Watanabe, et al. A case of pedunculated basal cell carcinoma on the right preauricular region. 2022; 76: 67-72.
- SP Walls, O Akinboboye, I Opoku, et al. Large fibroepithelial stromal polyp of the breast nipple. Cureus. 2022; 14: e26397.
- M Shaaban, EPL Turton, W Merchant. An usual case of a large fibroepithelial stromal polyp presenting as a nipple mass. BMC Research Notes. 2013; 6: 345.
- K Arora. A clinical case of large fibroepithelial polyp of breast nipple. Int J Rep Images. 2019: 10.
- V Banga, S. Jain. Fibroepithelial polyp (Acrochordon) of breast nipple – A rare clinical presentation. IP Archives of cytology and histology Research. 2022; 7: 54-56.
- K Belli, E Somuncu, T Aydogan, et al. Fibroepithelial polyp of the nipple in a woman. The Breast J. 2013; 19: 111-112.
- N Hirai, M Tamura. A case of giant fibroma pendulum of the labium majus group G streptococcal infection. Clinical Dermatology. 2010; 64: 235-238.
- M Husain, S Khan, A Bhat, et al. Accessory breast tissue mimicking pedunculated lipoma. BMJ Case Rep. 2014.
- P Singh, GM Anandani. Nevus lipomatousus superficialis, an unusual case report. J of Family Medicine and Primary Care. 2022; 11: 4045-4047.