Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 5
Open Access
Volume 5
Rami Ayoub1,2*; Omaymah Al-Shweiki3; Hassaan Bari1; Vandana Basappa Giriradder1; Ali Mohamedahmed1; Malik Kayal4; Jawad Ahmad1
*Corresponding Author: Rami Ayoub
Department of Hepatobiliary, University Hospitals Coventry & Warwickshire, UK.
Email: r.ayyoub@yahoo.com
Article Info
Received: Feb 10, 2025
Accepted: Mar 04, 2025
Published: Mar 11, 2025
Archived: www.jclinmedsurgery.com
Copyright: © Ayoub R (2025).
Abstract...
Gallstone disease is a common but its complications like Bouveret’s syndrome with Mirizzi syndrome are rare and can be life altering. We present a 64-year-old man who experienced a challenging course of gallstones. After a planned laparoscopic cholecystectomy that was abandoned due to concerns about gallbladder cancer, he developed gastric outlet obstruction caused by Bouveret’s syndrome which treated by Robotic-assisted gastrotomy that was successfully removed the three large gallstones from the stomach and the duodenum.
Repeat imaging showed residual gallstones in Hartmann’s pouch, with Type 4 Mirizzi syndrome. The patient then underwent robotic-assisted cholecystectomy with on table ICG assessment for bile leak and OGD to look for fistula and air leak, which both were normal.
On Postoperative day 2, patient developed peritonitis and started to drain biliary output in drains. He was taken to theatre for laparoscopic wash out and placement of large bore drains. Per operatively, undigested food was found in the porta hepatis, again no obvious source of bile leak or gas leak was found (there must be a small hole on both duodenum and bile duct which was not visible) MRCP showed bile duct was intact.
Patient was manged with NBM and TPN. The drain output was initially of duodenal contents but then started to become clear bile. ERCP was performed that showed bile leak at cystic duct area. Covered metal stent was placed, bile leak stopped. Patient discharged when he was eating and drinking well. Stent was removed 3 months later after MRCP which was clear. Patient recovered completely, following advanced surgical techniques, endoscopic interventions, and multidisciplinary care.
This case highlights the complexities of managing Bouveret’s syndrome, with a focus on the importance of innovative surgical approaches and collaborative care. A review of the relevant literature is also included.
Citation: Ayoub R, Al-Shweiki O, Bari H, Giriradder VB, Mohamedahmed A, et al. Management of Complex Gallstone Disease with Bouveret’s and Mirizzi Syndrome: A Case Report with Literature Review. J Clin Med Surgery. 2025; 5(1): 1185.
Introduction
Gallstone disease, a common gastrointestinal disease with a global adult population prevalence up to 20% [1], often necessitates cholecystectomy in symptomatic cases. Although the majority of cases are asymptomatic, complications are well established and include acute cholecystitis, cholangitis and pancreatitis. It is very rare for gallstone disease to present as Bouveret’s syndrome, a phenomenon characterized by gastric outlet obstruction secondary to migration of gallstones through a cholecystoenteric fistula [2]. This or similar conditions account for less than 3% of gallstone-related intestinal obstructions, and pose a diagnostic and therapeutic challenge [3].
Bouveret’s syndrome usually occurs in elderly patients with chronic cholecystitis and is characterized by symptoms of gastric outlet obstruction including continual vomiting, abdominal pain and weight loss [4]. Diagnosis is based on imaging modalities such as CT and endoscopy, which aid in identifying ectopic gallstones, and determine the obstruction [5]. For patients with larger or impacted stones or those with significant inflammation, surgical intervention is often needed. Management often starts by endoscopic removal of the stone [6].
Recent research from Chatterjee and De (2024), Ranjan et al. (2024), highlight the ever-growing role of advanced surgical and endoscopic techniques in the management of complex cases like Bouveret’s syndrome that have led to improved outcome [1,7,8].
We present an interesting case of a 64-year-old man diagnosed with Bouveret’s syndrome, Mirizzi syndrome, and a cholecystoduodenal fistula. Through this case and literature review, we hope to highlight the diagnostic and management challenges of rare complications of gallstone disease.
Case presentation
A 64-year-old male with past medical history of hypertension, ischemic heart disease, and obstructive sleep apnea presented with chronic abdominal pain and intermittent nausea secondary to gallstone disease. He was planned for a laparoscopic cholecystectomy at our hospital. During surgery, a suspicious mass in the gallbladder was found, and the operation was aborted owing to malignancy fears. Later biopsies, imaging and MDT discussion suggested chronic cholecystitis not cancer.
The patient subsequently developed acute gastric outlet obstruction and was unable to tolerate oral intake and developed persistent vomiting. A CT scan showed a large gallstone in the stomach consistent with Bouveret’s syndrome (Figure 1). He had robotic-assisted gastrotomy, at which point three large gallstones were removed successfully from the stomach and duodenum. The postoperative course was uncomplicated.
The subsequent MRI revealed a massive residual gallstone in Hartmann’s pouch leading to Type 4 Mirizzi syndrome and a cholecystoduodenal fistula (Figure 2). This led to a robotic-assisted subtotal cholecystectomy due to complex adhesions and distorted anatomy. Intraoperatively, he was found to have multiple adhesions with distorted anatomy. The obstructing stone was removed with subtotal cholecystectomy, ICG test showed no bile leak present at that time. In addition, the upper endoscopy during the operation showed the presence of a fistula.

Figure 1: Cholecytoduodenal fistula secondary to chronic calculous, Thick-walled gallbladder containing multiple gallstones with pericholecystic stranding. This appears continuous with a thickened duodenum which also appears to contain a gallstone. The stomach is distended with fluid and the downstream bowel loops are collapsed.
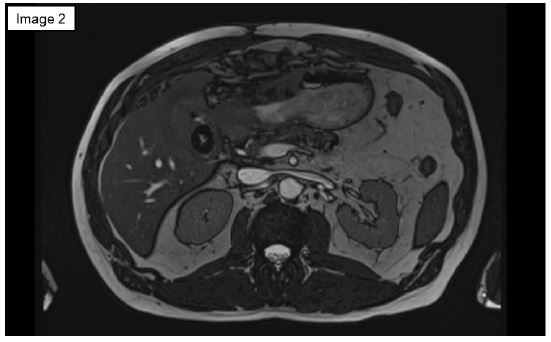
Figure 2: Pre operation MRCP: Choledochoduodenal fistula. Remnant gallstone in a nondistended inflamed gallbladder.
The patient experienced peritonitis and bile leakage in postoperative period. He underwent emergency laparoscopic washout and drain insertion, the laparoscopic surgery showed undigested food in the peritoneal cavity, likely due to leakage from the fistula and bile leak. Total Parenteral Nutrition (TPN) and other supportive care were provided to manage the output of the fistula.
A later MRCP and CT scan showed increased collection size, see (Figure 3). Iniatlly, US guided drain was inserted followed by ERCP, which showed a cystic duct leak, to insert a covered metal stent (Figure 4).
Gradually the patient stabilized, with all of the drains removed over time, and he was discharged home in good health.
On follow-up visit at 3 months, patient underwent ERCP for stent removal. Imaging confirmed an intact biliary tree without residual stones or leaks. He is now back to normal activity.
Literature review and discussion
Bouveret’s syndrome Firstly described by Leon Bouveret in 1896. It is defined by gastric outlet obstruction secondary to the passage of one or more gallstones via a cholecystoenteric fistula into the gastrointestinal tract. This rare condition accounts for less than 3% of all cases of gallstone ileus, but the atypical presentation and complexity of the intervention present significant diagnostic and therapeutic challenges [3].
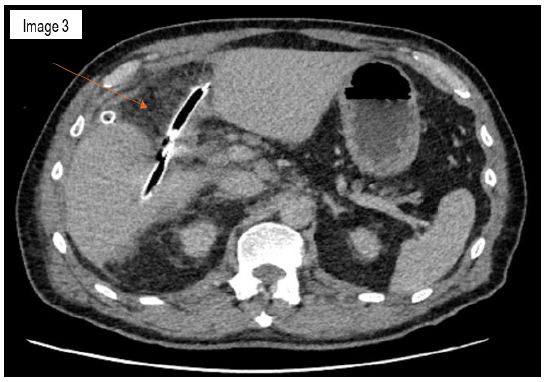
Figure 3: Subcapsular collections along the posterior medial subcapsular aspect of segment 6 and 7. There are multiple locules of air within the fluid suggests a gas forming component to the collection.
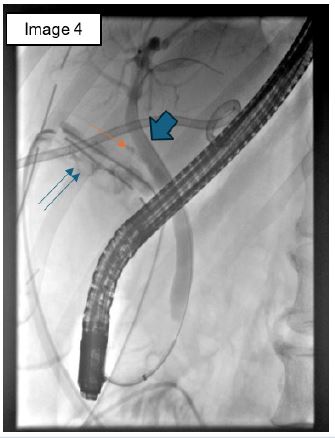
Figure 4: ERCP showed bile leak from the cystic duct. small one arrow: cystic duct, small 2 arrows: bile leak, large single arrow: CBD.
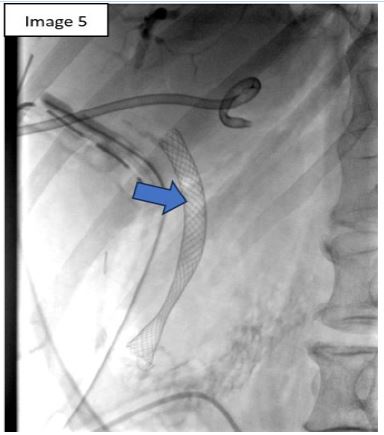
Figure 5: Metailc stent.
Globally, between 1967 and 2016, only 315 cases of Bouveret’s syndrome were reported in the medical literature. More recent reviews suggest approximately 550 to 600 cases have been documented to date, emphasizing its rarity and the need for heightened clinical awareness for timely diagnosis and management [9,10]. The most recent published papers are summarized in (Table 1).
The clinical presentation of Bouveret’s syndrome is generally nonspecific, with symptoms such as projectile vomiting, abdominal pain, and weight loss. These signs and symptoms can mimic those of other potential causes of gastric outlet obstruction, including malignancy or peptic ulcer disease, resulting in difficulty diagnosis [5]. Bouveret’s syndrome is diagnosed with imaging and endoscopy. Osman et al. highlighted the role of contrast- enhanced Computed Tomography (CT), which demonstrates ectopic gallstones, pneumobilia, and gastric outlet obstruction [6]. Endoscopy is key diagnostic tool, allowing not only for visualization but also for therapeutic intervention. Malik et al. highlighted the increasing importance of advanced imaging techniques and endoscopic modalities in early case diagnosis and definitive treatment [4].
Although a stepwise approach is recommended in the management of Bouveret’s syndrome, both endoscopic and surgical intervention would need to be employed for successful therapy. The gold standard treatment for gallstone disease is endoscopic removal, in particular for smaller stones. Larger or impacted stones require surgical intervention as stated by Smith et al. If enterotomy is not possible, alternatives may include gastrotomy or enterolithotomy using minimally invasive or robotic-assisted techniques to reduce postoperative morbidity [3,4]. Bouveret’s syndrome has a variable prognosis that depends on the timing of diagnosis and adequacy of treatment. Ranjan et al. reported that late intervention frequently results in complications including perforation, sepsis and prolonged hospital stay. The multidisciplinary approach to this problem should involve surgeons, gastroenterologists and radiologists to optimize outcomes. Resolution of this case, with robotic-assisted surgery and endoscopic stenting, highlights the value of tailored care plans and advanced treatments [8].
Bouveret’s syndrome is an uncommon condition but exemplifies the diagnostic and therapeutic challenges presented by complex gallstone disease. Recent advances in imaging modalities, endoscopic techniques and minimally invasive surgical approaches have all contributed to the markedly improved outcomes seen in these patients. As demonstrated in this case report, the use of these modalities in a multidisciplinary care context is critical for managing Bouveret’s syndrome optimally.
Table 1: Summary of studies on bouveret’s syndrome.
| Year | Title | Key Findings | Reference |
|---|---|---|---|
| 2024 | Bouveret’s syndrome: A rare presentation of a common surgical enigma | Discussed a caseof Bouveret’s syndrome, emphasizing diagnosticchallenges and management strategies. | [1] |
| 2024 | Management of complicated Bouveret’ssyndrome | Presented a case involving a large gallstonecausing gastricoutletobstruction, highlighting surgical management after unsuccessful endoscopic attempts. | [2] |
| 2023 | Bouveret's Syndrome: A Case Reportand Review of the Literature | Detailed a caseof an elderly woman with gastric outletobstruction due to a cholecystogastric fistula, emphasizing the challenges in management and the frequent need for surgical intervention. | [3] |
| 2021 | Bouveret syndrome: a rare causeof gastric outletobstruction | Reported a case of a 73-year-oldman with Bouveret’s syndrome, discussing the role of imagingand surgical intervention. | [4] |
| 2021 | Bouveret syndrome—arare form of gastric outletobstruction | Detailed a caseof a 90-year-old man, focusingon diagnostic modalities andtreatment options. | [5] |
| 2020 | Bouveret’s syndrome andcholecystogastric fistula: a case- report and review of the literature | Presented a case involving a cholecystogastric fistula, discussing the rarityof the condition and the need for surgical intervention after failed endoscopic attempts. | [6] |
| 2020 | Bouveret’s Syndrome – A Case Report and Reviewof Literature | Discussed a case of Bouveret’s syndrome in a79-year- old woman,emphasizing the importance of imaging and thechallenges in diagnosis and management. | [7] |
| 2019 | Acase report and review of the literatureof Bouveret syndrome | Illustrated the severity of Bouveret syndrome through a casestudy, reviewing various endoscopic and surgical treatment methods. | Singh G, Merali N, Shi- rol S, Dr mousis P, Singh S, Veeramootoo D. Ann R Coll Surg Engl. 2020;102: e15-e19. |
| 2012 | Bouveret's syndrome: a case reportanda review of the literature | Presented a case of an elderly woman with Bouveret's syndrome, discussing the surgical management and reviewing relevant literature. | Lee W, Han SS, Lee SD, et al. KoreanJ Hepatobiliary Pancreat Surg. 2012; 16: 84–87. |
Conclusion
Bouveret’s syndrome is a rare but significant and intricate complication of gallstone disease. This case highlights the vital role of advanced imaging, surgical innovation, and multidisciplinary collaboration in successfully managing complex conditions.
A combined approach, utilizing both endoscopic and surgical techniques, is often critical for effective treatment. However, even with meticulous surgical planning, complications such as post-operative bile leaks and peritonitis may arise. Addressing these challenges requires diligent, day-by-day follow-up and comprehensive recovery care to achieve optimal outcomes.
References
- Chatterjee I, De U. Bouveret’s syndrome: a rare presentation of a common surgical enigma. J Surg Case Rep. 2024; 2024: rjae379.
- Ranjan P, Jha VC, Gopal P, Banerjee D. Management of complicated Bouveret’s syndrome. BMJ Case Rep. 2024; 17: e261232.
- Malik S, Khan H, Bapaye J, Mushtaq A. Bouveret’s Syndrome: A Case Report and Review of the Literature. Adv Clin Med Res Healthc Deliv. 2023; 3.
- Smith C, Singh S, Vulliamy P, Mukherjee S. Bouveret syndrome: a rare cause of gastric outlet obstruction. BMJ Case Rep. 2021; 14: e240236.
- Jin L, Naidu K. Bouveret syndrome—a rare form of gastric outlet obstruction. J Surg Case Rep. 2021; 2021: rjab183.
- Osman K, Maselli D, Kendi AT, Larson M. Bouveret’s syndrome and cholecystogastric fistula: a case- report and review of the literature. Clin J Gastroenterol. 2020; 13: 527-531.
- Al-Saadi H, Okeke I, Mathew SS, et al. Bouveret’s Syndrome – A Case Report and Review of Literature. Clin Surg J. 2020; 1.
- Ranjan P, Jha VC, Gopal P, Banerjee D. Advanced techniques in Bouveret’s syndrome management. BMJ Surg Innov. 2024; 12: e285032.
- Awan F, Dar FS, Haider R. Trends in the global incidence of Bouveret’s syndrome: a systematic review. World J Gastrointest Surg. 2016; 8: 253-262.
- Gupta P, Sharma S, Chatterjee N. A rare complication: Bouveret’s syndrome revisited. Int J Surg Case Rep. 2023; 19: 224-230.