Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Jing Niu, MD1; Li Shen, MD1; XuBai Qiao, MD2; Yao Feng, MD1; Lu Jike, MD, PhD1*
*Corresponding Author: Lu Jike, MD, PhD
Department of Orthopedic Surgery, Beijing United Family Hospital, No 2 Jiangtai Road, Chaoyang District, Beijing, 10016, China.
Email: jike.lu@ufh.com.cn
Article Info
Received: Dec 01, 2024
Accepted: Jan 02, 2025
Published: Jan 09, 2025
Archived: www.jclinmedsurgery.com
Copyright: © Jike L (2025).
Abstract...
Lipoma arborescens is a rare and benign intra-articular lesion characterized by villous lipomatous proliferation of the synovium, usually involving the suprapatellar pouch of the knee joint. It is an uncommon cause of intra-articular masses that presenting as slowly progressive painless swelling of the joint, which persists for many years and is accompanied by intermittent effusions. It is not a neoplasm, but rather considered to be a nonspecific reactive response to chronic synovial irritation, whether from mechanical or inflammatory insults. The cause of lipomas is often unknown, but some families have a genetic predisposition to develop them. They are more common in patients aged 40 to 60 years. Lipoma arborescens is supposed to originate within the joint, either by penetrating the synovial membrane or by fatty overgrowth from the intra-articular synovial tissues. It presents as an unusual cause of intermittent knee pain, mechanical locking symptoms, and joint effusion.
We report a case of lipoma arborescens of the knee in a 30-year-old man that initially resembled inflammatory arthropathy. The diagnosis of lipoma arborescens was made by Magnetic Resonance Imaging (MRI) of the knee and confirmed histologically by arthroscopically assisted synovectomy.
Keywords: Lipoma arborescens; Knee; Arthroscopy; Mechanical symptoms; MRI.
Citation: Niu J, Shen L, Qiao X, Feng Y, Jike L. Unusual Lipoma Arborescens of the Knee with Mechanical Locking Symptoms: A Case Report. J Clin Med Surgery. 2025; 5(1): 1179.
Introduction
Primary lipoma arborescens in the synovium is not common and usually presents as benign, tumor-like lesions. Lipoma arborescens is characterized by the proliferation of mature adipocytes within the joint synovium. Although it is an idiopathic disorder, chronic mechanical disease, and synovial inflammation are thought to potentially trigger this rare proliferative disorder.
Despite its low incidence, lipoma arborescens remains a diagnostic challenge due to its similarity to other joint disorders, which may lead to misdiagnosis and delayed treatment [1-3]. Accurate diagnosis requires a multidisciplinary approach, including clinical evaluation, advanced imaging modalities, and histopathological analysis. MRI is the diagnostic modality of choice, due to its high sensitivity to fatty tissue. The identification of villous-lipomatous synovial proliferation is pathognomonic for lipoma arborescens. Arthroscopically surgical synovectomy is one of primary therapeutic options.
Case presentation
A 30-year-old man, complained of swelling in the left knee persisting for 2 months, associated episodes of joint effusion. The pain was insidious in onset, aggravated by squatting and prolonged sitting. He has mechanical symptoms such as catching and locking symptoms of the knee and significantly reduced knee range of the movements, especially flexion less than 90 degrees, and fixed flexion deformity of the knee was about 30 degrees. There was a diffuse swelling of the left knee predominantly on the medial infrapatellar close to trochlea groove which was doughy in consistency with limited range of movements. Additionally, the patient also reported he has right shoulder pain for last three months which was debilitated and significantly reduced range of movements. The patient did not benefit from several knee aspirations for ease of his knee large effusion. Despite treatments involving corticosteroid injections and nonsteroidal anti-inflammatory drugs, there was no significant improvement in symptoms. Subsequently, he was suggested to have surgical management.
Clinical examination revealed a diffuse and painful swelling in the suprapatellar region, with a patellar tap test positive, and infrapatellar fullness in the left knee and a limitation in right shoulder movements with pain were documented. The aspiration of the left knee did not reveal any evidence of crystals or sign of infection.
The MRI studies revealed several frond-like villi projecting into the joint from the synovium at infrapatellar region on sagittal view, exhibiting low signal T2 weighted (Figure 1A). No signs of meniscal or ligamentous lesions were seen. MRI axial image of the left knee shows a nodular frond-like intra-articular fatty mass at infrapatellar Hoffa fat pad close to trochlea groove with surrounding effusion, consistent with nodular lipoma arborescens which was causing mechanical symptoms (Figure 1B).
In our case report, MRI showed several frond-like villi projecting into the joint from the synovium over anterior distal femur, exhibiting high signal T1 weighted image (Figure 2A). MRI T-1 weighted sagittal and axial images of the left knee (Figure 2B) showed a nodular frond-like intra-articular fatty mass (arrow) at infrapatellar Hoffa fat pad close to trochlea groove with surrounding effusion, consistent with nodular lipoma arborescens that was causing mechanical symptoms and proved that after surgery all mechanical symptoms disappeared.
Further confirmed from MRI, intra-articular lesion characterized by villous lipomatous proliferation of the synovium, usually involving the suprapatellar pouch of the knee joint. T1-weighted images demonstrate several intermediately signaled frond-like villi projecting into the joint from the synovium of the anterior distal femur at suprapatellar pouch with effusion (Figure 3A and B).
Arthroscopically assisted synovectomy and resection of hypertrophic synovial tissue were performed. Arthroscopically assisted excision of the frond-like villi which were just in front of the ACL ligament and in suprapatellar pouch (Figure 4A and B). At the same time, arthroscopically assisted excision of villi-like lipoma arborescens was performed in shoulder joint as well (Figure 5). Histologic examination confirmed the diagnosis of lipoma arborescens (Figure 6). Pathology study showed reactive hyperplastic changes with marked chronic inflammation, mature adipocytes proliferation and replacing sub synovial connective tissue (Figure 6). The histologic changes are consistent with synovial lipomatosis of his MRI findings. No evidence of malignancy was seen. His knee pain and catching locking symptoms were completely relieved in 3, 6 months postoperatively follow up.
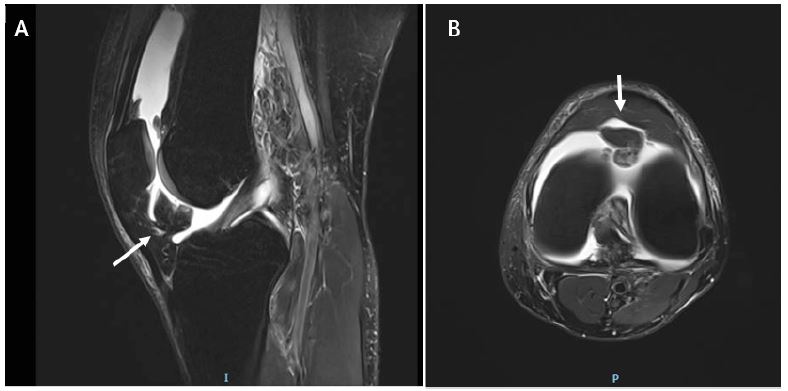
Figure 1: The MRI revealed several frond-like villi projecting into the joint from the synovium at infrapatellar region on sagittal view (an arrow), exhibiting low signal T2 weighted (Figure 1A). No signs of meniscal or ligamentous lesions were seen. MRI axial image of the left knee show a nodular frond-like intra-articular fatty mass (arrow) at infrapatellar Hoffa fat pad close to trochlea groove with surrounding effusion, consistent with nodular lipoma arborescens which was causing mechanical symptoms (Figure 1B).
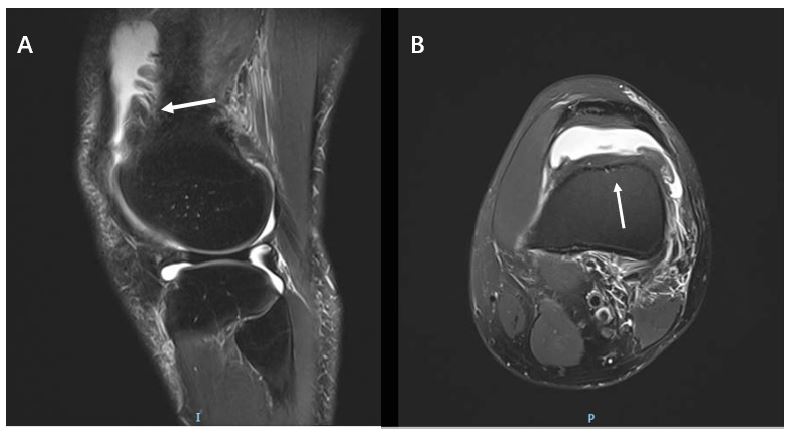
Figure 2: The MRI showed several frond-like villi projecting into the joint from the synovium over anterior distal femur, exhibiting high signal T1 weighted image (an arrow in A). MRI T-1 weighted sagittal and axial images of the left knee (B) showed a nodular frond-like intra-articular fatty mass (arrow) at infrapatellar Hoffa fat pad close to trochlea groove with surrounding effusion, consistent with nodular lipoma arborescens that was causing mechanical symptoms and proved that after surgery all mechanical symptoms was disappeared.
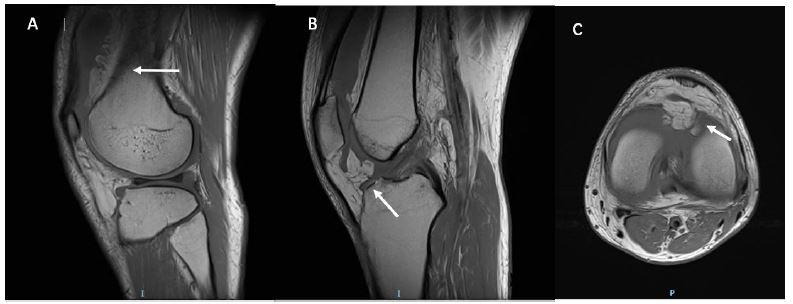
Figure 3: MRI intra-articular lesion characterized by villous lipomatous proliferation of the synovium, usually involving the suprapatellar pouch of the knee joint. T2-weighted images demonstrate several low signal frond-like villi projecting into the joint from the synovium of the anterior distal femur at suprapatellar pouch with effusion (Figure 2A & B).
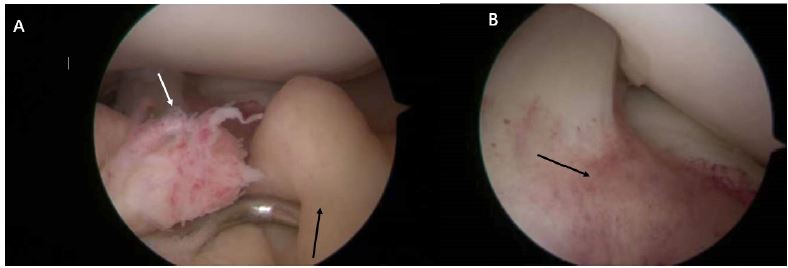
Figure 4: Arthroscopically, the subsynovial fatty proliferation in lipoma arborescens can be focal nodular frond-like adipose synovium tissues (arrows in A), After arthroscopically assisted excision of the frond-like villi which were just in front of the ACL ligament (an arrow in B).
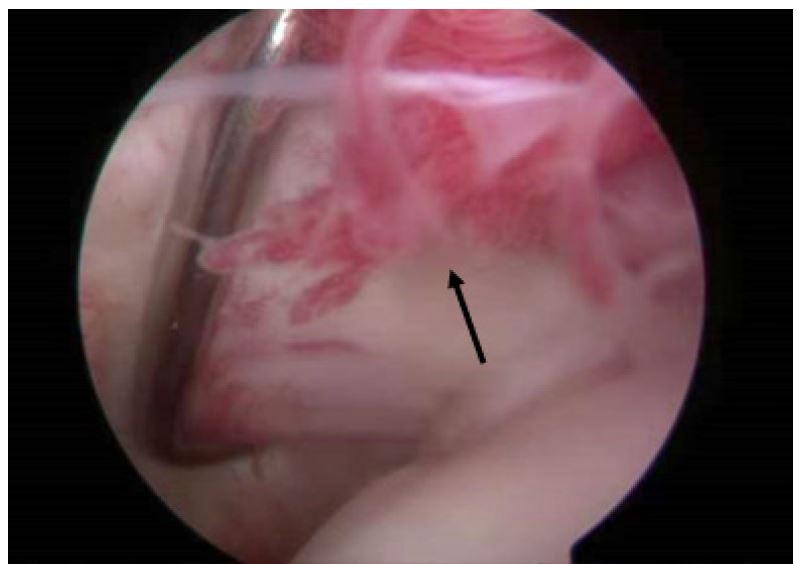
Figure 5: Arthroscopically assisted excision of villi-like lipoma arborescens was performed in shoulder joint (an arrow).
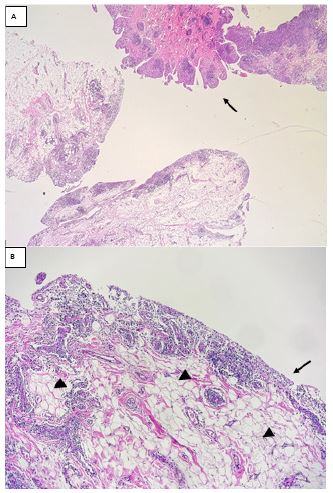
Figure 6: Histology section show several papillaroid structures and reactive hyperlastic changes with a remarkable chronic inflammation (an arrow in A), the papillaroid structure with synovial lining cells (an arrow in B) with inside mature adipocytes proliferation (arrow heads in B) and replacing subsynovial connective tissue [Haematoxylin & eosin (A) × 2; (B) × 10].
Discussion
Lipoma arborescens is a rare synovial disorder of unknown etiology and characterized by a villous lipomatous proliferation of the synovial tissue. It reaches adults between the fifth and seventh decades [1-3]. Men and women are equally affected. It is a chronic, slow growing intra-articular benign lesion. The knee joint, preferentially the suprapatellar pouch, is the preferred site for the lipoma arborescens, although other joints such as the hip, elbow, shoulder, and ankle have been described. While the condition primarily manifests unilaterally, instances of multiple, and bilateral joint involvement have also been documented [1-3].
There are two types of lipoma arborescens. The primary type, considered rare, manifests spontaneously without any prior degeneration of the knee joint. On the other hand, the secondary type is more frequent and characterized by synovial lipomatosis associated with underlying chronic irritation, such as osteoarthritis, meniscal injury, trauma, arthritis, or chronic synovitis [1-4].
Clinical presentations typically include long-lasting and slowly progressive joint pain, swelling with recurrent effusion, possibly mechanical catching, locking symptoms as our case complained. The worsening of clinical manifestations may be related to the entrapment of hypertrophic villi between the moving joint surfaces. Laboratory tests, including erythrocyte sedimentation rate, rheumatoid factor serology, and uric acid levels, are in normal ranges. Joint aspirates are negative for crystals and synovial fluid cultures.
Precise confirmation of lipoma arborescens requires a thorough physical and image examinations. Imaging techniques such as MRI is essential in identifying the characteristic signs of fatty tissue proliferation in the synovial space. The MRI characteristics of lipoma arborescens includes a synovial mass with an arborescent frond-like structure in the pre-femoral area and infrapatellar region (Figures 1,2). This mass typically demonstrates signal intensity similar to that of fat crossing all pulse sequences. Contrast administration, the hypertrophied subsynovial fatty tissue typically remains unenhanced, whereas the chronically inflamed overlying thickened synovium often displays diffuse enhancement [5,6].
Additionally, degenerative changes and meniscal tears can be noted as pathological factors contributing to the development of lipoma arborescens.
Although radiographs have limited value in the diagnosis of lipoma arborescens, it can show soft tissue shadow in the suprapatellar recess, often associated with osteoarthritic changes in the secondary form.
Lipoma arborescens forms part of the differential diagnosis [7-9] of a chronic joint swelling; including pigmented villonodular synovitis, synovial osteochondromatosis, rheumatoid arthritis, intra-articular or synovial lipoma, synovial hemangioma, amyloid arthropathy, and xanthoma. Intra-articular lipoma and synovial osteochondromatosis are the only among these entities that can demonstrate similar MRI signal characteristics.
Intra-articular lipoma can be differentiated from lipoma arborescens based on its gross and microscopic features. It appears as a solitary round or oval mass, as opposed to the multiple villous lipomatous proliferations and the frond-like morphology of lipoma arborescens. Intra-articular synovial lipoma is composed of mature fat cells covered by a thin fibrous layer, usually with no synovial lining. Histologically, lipoma arborescens is characterized by diffuse replacement of the subsynovial layer by mature fat cells with a moderate infiltration of mononuclear cells (Figure 6). Synovial osteochondromatosis is characterized by a nodular proliferation and metaplasia of the synovial membrane. On MRI, the signal intensity of it is similar to that of lipoma arborescens, but because of the cartilaginous nature of the lesion and the extent of the ossified or calcified regions, the signal intensity usually varies. In addition, the calcified or ossified lesions usually can be seen on radiographs.
Synovial hemangioma is a benign vascular malformation of the synovium which mainly occurs in children and adolescents. MRI demonstrates a lobulated intra-articular mass with a hyper intense signal due to pooling of blood in vascular spaces. Furthermore, lipoma arborescens usually arises in the suprapatellar pouch, whereas a synovial hemangioma is primarily found in the infrapatellar pad. In our case report, exceptionally, lipoma aborescens found either in suprapatellar pouch or infrapatellar region (Figures 1-3)
Joints affected with chronic rheumatoid arthritis show diffuse joint space loss, periarticular osteopenia, soft-tissue swelling, and marginal erosions on plain radiographs. Chronic rheumatoid arthritis has intermediate to low signal intensity on T1- and T2-weighted MRI-images associated with the formation of fibrous pannus. When affecting multiple joints, lipoma arborescens can mimic rheumatoid arthritis; but history, physical examination, laboratory tests, and radiography allow us to distinguish between rheumatoid arthritis and lipoma arborescens.
The definitive diagnosis of arborescent lipoma is typically established through histopathological examination, obtained by synovial tissue biopsy or surgical intervention [9]. Microscopic analysis reveals the presence of mature adipocytes infiltrating the subsynovial tissues (Figure 6), distinguishing it from other joint pathologies.
The treatment of lipoma arborescens is essentially based on surgical or arthroscopically assisted synovectomy, which is the main therapeutic approach aimed at removing proliferative or blocking adipose tissues and restoring joint function. Arthroscopically assisted synovectomy offers a minimally invasive approach, facilitating early postoperative recovery compared to open surgery.
Conclusion
In summary, lipoma arborescens presents as a rare benign intra-articular lesion primarily observed in the knee joint. It warrants consideration in cases of chronic joint swelling, whether accompanied by pain, mechanical symptoms or not. MRI stands out as the preferred imaging technique for diagnosing this condition, owing to its exceptional ability to differentiate fatty tissue with high sensitivity. Early arthroscopically assisted synovectomy is the optimal surgical approach, allowing quicker, better functional outcomes.
References
- Hallel T, Lew S, Bansal M. Villous lipomatous proliferation of the synovial membrane (lipoma arborescens) J Bone Joint Surg Am. 1988; 70: 264–70.
- De Vleeschhouwer M, Van Den Steen E, Vanderstraeten G, et al. Lipoma arborescens: review of an uncommon cause for swelling of the knee. Case Rep Orthop. 2016, 2016: 9538075.
- Lyrtzisa C, Stamati A, Pantazis E, et al. Lipoma arborescens of the knee: A case report and comprehensive review. Medical Reports. 2023; 1: 100021.
- Baidoo PK, Nketiah-Boakye F, Tano EK, et al. Lipoma arborescens in a 16-year-old male: A case report. Clinical Case Reports. 2021; 9: e05230.
- Patil PB, Kamalapur MG, Joshi SK, et al. Lipoma arborescens of knee joint: role of imaging. J Radiol Rep. 2011; 5: 17–25.
- Soler T, Rodríguez E, Bargiela A, et al. Lipoma arborescens of the knee: MR characteristics in 13 joints. J Comput Assist Tomogr. 1998; 22: 605-609.
- Chahdi HO, Bouardi N EI, Ferhi M, et al. Lipoma arborescens of the knee: A case report Radiology. Case Reports. 2024; 19: 2272-2276.
- Patil PB, Kamalapur MG, Joshi SK, Dasar SK, Rao RV. Lipoma arborescens of knee joint: role of imaging. J Radiol Case Rep. 2011; 5: 17–25.
- Drevelegas A, Pilavaki M, Chourmouzi D. Lipomatous tumors of soft tissue: MR appearance with histological correlation. Eur J Radiol. 2004; 50: 257-267.