Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Seyed Farzad Maroufi1,2; Mohammad Amin Dabbagh Ohadi1; Hanan Ebrahimi1; Hadi Digaleh1; Arad Iranmehr1; Mohammad Reza Keshavarz Darolkalaei3; Amin Jahanbakhshi3,4; Mostafa EL Khashab5; Zohreh Habibi1; Farideh Nejat1; Keyvan Tayebi Meybodi1*
*Corresponding Author: Keyvan Tayebi Meybodi
Department of Neurosurgery, Tehran University of Medical Sciences, Tehran, Iran.
Tel: +989127997920;
Email: Ktayebi@gmail.com
Article Info
Received: Nov 23, 2024
Accepted: Dec 20, 2024
Published: Dec 27, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Tayebi Meybodi K (2024).
Abstract...
Introduction: The position of the ventricular catheter tip is critical to shunt success, but few publications regarding analytical validation of entry points and trajectories for ventricular access can be found in the literature. No validated data exists on entry points and trajectories for ventricular catheter insertion in pediatric populations due to differences in head size or age. This study seeks to define a new entry point for normal pediatric populations based on simple demographic data.
Method: Multi-slice CT scans were performed on 32 pediatric patients who had two intact lateral ventricles. The study used a bisector-defined trajectory line to determine the entry point, entry angle, and parenchymal mantle. Statistical analysis was performed to develop a model for identification of craniometrics dimensions of posterior ventricular access. The model was validated by calculating the success rate of ventricular entry using the proposed trajectory line in another sample.
Results: The study found that age was significantly correlated with posteriority and parenchymal mantle, while sex was significantly associated with superiority. A multivariate regression model identified the best-fit equation for predicting entry point characteristics, which were then used to calculate entry points for the validation sample. The success rate of the entry points was 93.55%, and mean parenchymal mantle did not differ significantly from the main sample.
Conclusion: An equation-based model was proposed to define the craniometric dimensions of posterior entry point for ventricular access in pediatric population. The model was proved to transgress the least parenchymal mantle. Also, more than 90% success rate of the model to enter into the ventricular cavity makes it a relatively suitable one for young surgeons to accurately insert a posterior ventricular catheter.
Keywords: Ventricular access point; Craniometric points; Pediatric population; Mathematical model; Parenchymal mantle; Success rate.
Citation: Farzad Maroufi S, Dabbagh Ohadi MA, Ebrahimi H, Digaleh H, Tayebi Meybodi K, et al. A Mathematical Model for Identification of Craniometric Dimensions of Posterior Ventricular Access in Pediatric Population. J Clin Med Surgery. 2024; 4(2): 1178.
Introduction
It is more than 80 years that the first clinically successful shunts, improvised by Arne Torkildsen, have been used as the treatment for hydrocephalus [1]. Since then, despite improvement in many aspects of hydrocephalus and its management, no major advancement has been achieved in shunt survival, as so far, more than one-third of shunt failures occur in the first year after shunt implantation [2,3].
As many as one-third of the shunt malfunctions are due to ventricular catheter obstruction [3,4]. Brain debris, and ependymal or choroid plexus ingrowth are major etiologies of ventricular catheter obstruction [5]. Therefore, the position of the ventricular catheter tip (the hole-bearing segment of the catheter) plays a vital role in the fate of the shunt. The ventricular catheter tip is theoretically determined by ventricular catheter entry point, catheter trajectory, and catheter length, all of which are modifiable factors among the indefinite number of factors that influence VP shunt survival. Although multiple entry points with various trajectories have been formerly proposed for ventricular access through the posterior skull, but, to the best of our knowledge, none of them have been analytically validated regarding success rate for ventricular access, complication rate, or effect on shunt survival.
Although there is immense clinical data regarding ventriculoperitoneal shunt outcomes in the pediatric population, few publications on the precise ventricular catheter entry points or their trajectories in the pediatric population can be found in the literature [6,7]. Apparently, the craniometric dimensions of entry points that have been defined in the adult population cannot be used in the pediatric population due to smaller heads. In this study, we tried to define a new posterior entry point in relation to head circumference and age of the normal pediatric population.
Material and methods
This study was approved by the ethical council of Tehran University of Medical Science (IR.TUMS.MEDICINE.REC.1398.654). 32 pediatric patients, who underwent brain CT because of head trauma were consecutively enrolled as the main sample in this study. The indication for CT was determined by the staff physicians at emergency department of Children’s Medical Center. Multi-slice CT scans with overlapping sections of 1.25 mm were performed, according to the standard protocol of the center, to rule out intracranial pathology. The images were obtained in the orbitomeatal plane, which was defined as a line in the scout image passing through the anterior orbital roof and external auditory meatus. All had two intact lateral ventricles. No patient had intraventricular mass, midline shift, porencephaly, mass effect, history of the previous craniotomy, clinically noticeable congenital skull anomaly, or skull or scalp defect. Age and head circumference was also recorded for all participants. Informed consent was obtained from the patients’ guardians to use the data for research purpose.
Determination of entry point was done according to our previous study [8]. In summary, the slice in which the external auditory canal had maximal length was chosen, and the anterior-most, lateral point of the canal was defined as the “reference point” (Figure 1). Then, scrolling from rostral to caudal, the inferior-most slice in which both thalami were not seen was chosen as the “entry plane” (Figure 2). The interception of the bisector of the angle defined by the tangent lines to the medial and lateral atrial walls with scalp and skull was named the “entry point”. The bisector was defined as the “trajectory line” (Figure 2), and the obtuse angle between this line and the tangent line to the scalp was named the “entry angle” (Figure 3). The distance between the interception points of the “trajectory line” to the external table of the skull and the atrium was defined as the “parenchymal mantle” (Figure 3). Then the Cartesian dimensions of the “entry point” in reference to the “reference point” were measured in millimeters.
Statistical analysis
R program (version 4.1.2) was used for statistical analysis. In order to evaluate correlations between different variables and their significance, the rcorr function was used, followed by multiple-comparison correction by Bonferroni correction. We further used stepwise Akaike Information Criterion (AIC) model selection in multivariate general linear regression using GLM, stepAIC, and aictab functions to generate the most accurate model [9]. Continuous variables were reported using mean and standard deviation and compared using independent sample T-test. P-value<0.05 was considered significant.
Validation
In order to validate the model, information on another set of patients who were referred to our center due to trauma was recorded. The exact age of the patients was calculated, and both superiority and posteriority were calculated using the developed model. Then, using the obtained measurements, the entry point was determined on both sides of the skull, and a line was drawn using the mean entry angle derived from the main sample group, from that point to the ventricle on the same side. This angle was the mean entry angle in the main sample group. The length of the line drawn from the inner surface of the skull to the ventricle was recorded in each case. Finally, the success of the model was calculated in terms of the percentage of successful ventricular entry by the proposed trajectory.
Results
Information and CT scans of 36 consecutive patients were recorded as the main sample of the study and were used to draw trajectory lines based on our previously discussed method [8]. 52.78% of the sample were male, and the mean age of the sample was 3.59±3.05 years. The mean parenchymal mantle was 31.12±4.36 mm and the mean entry angle was 74.24±5.56 degree. Analysis of bivariate relationships between demographic predictors and entry point craniometrics dimensions revealed that there is no relationship between the entry side (right or left) and the entry point craniometric dimensions; in other words, there was no difference between entry point characteristics on either site.
However, age has been significantly correlated with posteriority (r=0.42, p=0.00) and parenchymal mantle (r=0.44, p=0.00) (Table 1). Furthermore, HC has been significantly associated with parenchymal mantle (r=0.42, p=0.0), and sex with superiority (r=0.34, p=0.03). HC and posteriority (r=0.26, p=0.21) failed to correlate after controlling for the type 1 error rate.
The influence of demographic predictors and their interaction on the entry point characteristics was estimated using stepwise AIC model selection in multivariate general linear regression to identify the best-fit model among those describing the correlation (Table 2). Age explained 19% of the variance of the posteriority (F=17.03, p-value<0.001, adjusted R-squared: 0.19, β=1.21, AIC: 490.43). In addition, sex (β=5.9963, p-value<.0001) and age (β=1.6124, p-value<.0001) and their interaction (β= -0.8347, p-value<.001) accounted for 32% of the variation in the superiority (p-value<.001, F-statistic: 11.86, adjusted R-squared: 0.3206, AIC: 366.64). Detailed steps were provided in Table 3.
The final model resulted in the following equation:
Posteriority=1.21 ×Age+31.21
Superiority=(0.78×Age)+(6×Sex)+(-0.8347×Age×Sex)+53.25
Sex (Male: 1, Female: 2); Age (year) 32 consecutive patients were included in the validation phase of our study. Entry point location was calculated using the above equations. One of the patients had an unsatisfying brain CT scan and was excluded from further evaluation. Male patients comprised 58.06% of the validation sample. The mean age of the sample was 4.11±2.87 years (ranging from 0 to 9). The validation sample did not differ from the main sample in terms of age and sex (p=0.48, 0.66, respectively). Among 62 trajectory lines (one on each side of the skull), 58 reached the ventricle, resulting in a 93.55% success rate. Regarding the failed trajectories, one patient had failed entry on both sides, and the trajectory lines reached the opposing ventricles. In one of the cases, although the trajectory line reached the ventricle on one side, the ventricle could not be observed on the other side leading to a failed entry. In another case, on the left side, the trajectory line entered the space between to ventricles. Mean parenchymal mantle, in cases in which the trajectory line entered the ventricle, was 31.60±4.92 millimeters. The parenchymal mantle in validation group did not differ significantly from the main sample (p=0.55).
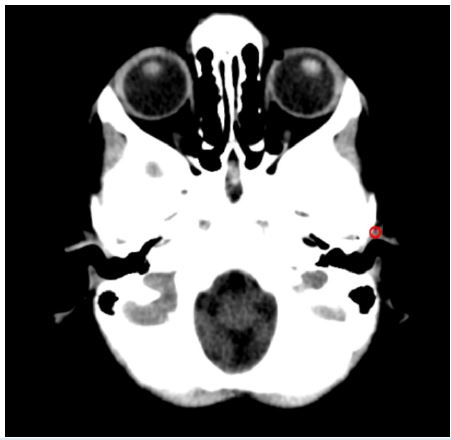
Figure 1: “Entry plane” is the plane in which the external auditory canal has the maximal length. Red circle shows the lateral, anterior-most point of the external auditory canal, which is named “entry point”.
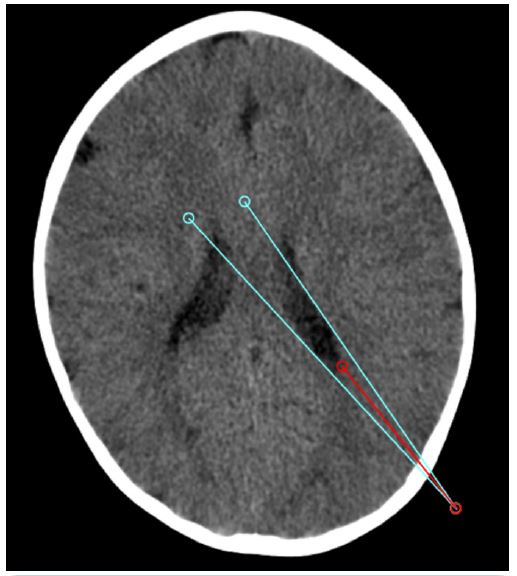
Figure 2: "Trajectory line” is the bisector of the angle created by the two tangent lines to the medial and lateral wall of the atrium. “Entry point” is the point of interception of the “trajectory line” to the outer table of the skull.
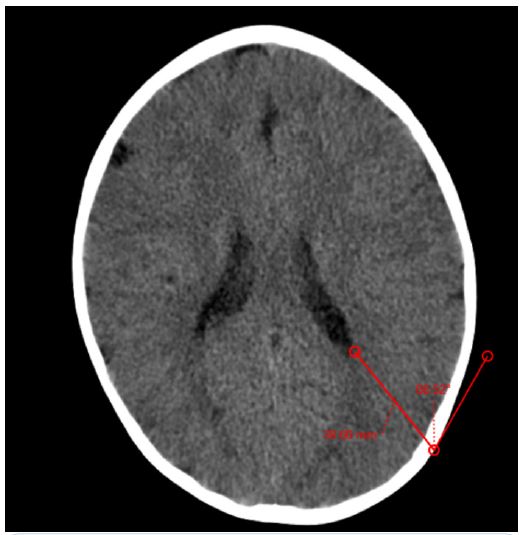
Figure 3: “Entry angle” is the obtuse angle produced by the interception of the “trajectory line” and the tangent line to the scalp.
Table 1: Bivariate relationship between demographic predictors and surgical point characteristics.
| Superiority (R, p-val) | Posteriority (R, p-val) | Mantle (R, p-val) | |
|---|---|---|---|
| HC | 0.16, 1.00 | 0.26, 0.21 | 0.42, 0.00*** |
| Side | 0.03, 1.00 | 0.09, 1.00 | 0.09, 1.00 |
| Age | 0.22, 0.44 | 0.42, 0.00*** | 0.44, 0.00*** |
| Sex | 0.34, 0.03* | 0.05, 1.00 | 0.01, 1.00 |
Table 2: Multivariable regression models were constructed to estimate surgical points using demographic variables. Only those combinations that estimates the best Akaike Information Criterion (AIC) were displayed.
| β | Lower 95% | Upper 95% | P-value | |
|---|---|---|---|---|
| Posteriority | ||||
| Intercept | 31.21 | 28.54 | 33.88 | <0.001 |
| Age | 1.21 | 0.63 | 1.78 | <0.001 |
| Superiority | ||||
| Intercept | 47.2580 | 43.5931014 | 50.9228126 | <0.001 |
| Age | 1.6124 | 0.8466763 | 2.3781505 | 0.0001 |
| Sex | 5.9963 | 3.6916870 | 8.3008191 | <0.001 |
| Age: Sex | -0.8347 | -1.3305245 | -0.3389666 | 0.001 |
| Angle | ||||
| Intercept | 74.24 | 72.95 | 75.52 | <0.001 |
| *Indicates an interaction relationship. | ||||
Table 3: Different combinations were assessed to find the best predictor for surgical entrance point using the AIC. We chose the model with the lowest AIC value as the best model.
| Model | AIC | AICc weight |
|---|---|---|
| Posteriority ~Age | 490.43 | 0.49 |
| Posteriority ~ Age + Side | 491.32 | 0.32 |
| Posteriority ~ Age + Side + HC | 492.92 | 0.14 |
| Posteriority ~ Age + Side + HC + Sex | 495.21 | 0.05 |
| Model | AIC | AICc weight |
| Superiority ~ Age + Sex + Age:Sex | 366.64 | 0.55 |
| Superiority ~ Age + Sex + Age:Sex + Side | 367.59 | 0.34 |
| Superiority ~ Age + Sex + Age:Sex + Side + HC | 370.03 | 0.10 |
| Superiority ~ Age+ Sex + Side + HC | 378.09 | 0.0 |
| Model | AIC | AICc weight |
| Angle~ 1 | 454.48 | 0.59 |
| Angle~ Side | 456.10 | 0.26 |
| Angle~ Side + HC | 457.90 | 0.11 |
| Angle ~ Side+ HC + Age | 460.07 | 0.04 |
| Angle ~ Side + HC + Age+ Sex | 462.45 | 0.01 |
| *Indicates an interaction relationship. | ||
Table 4: Previously proposed posterior entry points for ventricular catheterization. NA denotes “not available”.
| Point | Reference point | Entry point | Trajectory | Target | Population age by which the point has been defined | Success rate | Samples(cadaver/ radiology/realpatients) |
|---|---|---|---|---|---|---|---|
| Keen | External auditorymeatus | 1.25 inch superior and 1.25 inch posterior to external auditory meatus, in a plane perpendicular to Reid baseline | 2.5inch superior to contralateral meatus, perpendicular to Reid baseline | Atrium | Pediatrics | NA | Real patient |
| Dandy [14] | Inion | 3 cm abovethe inion and2 cm lateral to the midline. | Perpendicular to skull | Atrium | Adults | NA | Real patients |
| Frazier [14] | Inion | 6 cm superior to the inionand 3 cm lateral to the midline | 4 cm abovethe contralateral medialcanthus | Atrium | Adults | NA | Real patients |
| Kingsly [6] | Parietal boss | One fingerbreadth posteriorand inferior to the parietal boss | NA | Lateralventricle | Pediatrics | 98% | Real patients |
| Tayebi Meybodi [8] | External auditorymeatus | 57 and 51 millimeters Posterior,and60 and 58 millimeters above reference point | Parallel to orbitomeatal plane, with 77-78 degrees angle to a line tangent to the posterior skull | Atrium | Adults | 100% | Radiology of normal population |
| Duong [19] | NA | Midline distance between a patient’s Keen’s and Frazier’s point | 4 cm above thenasion | Atrium | Adults | 85% | Real patients |
Discussion
Currently, although ventricular shunts are used as one of the main treatments in children with hydrocephalus and increased intracranial pressure such as idiopathic intracranial hypertension, there are many challenges in choosing the point of entry into the skull and the angle of entry. Extensive studies have already been performed on adults, but these studies are very limited in pediatrics population. Especially in children, due to age-related skull growth, an absolute point may not be ideal for different individuals. In our previous report, we defined a new entry point for posterior ventricular access in adults, which has been suggested to have less technical failure in comparison to Keen and Frazier’s points. Moreover, this point traversed less brain parenchyma than the two historical points [8]. The aim of this study, which to our best of knowledge is the first in its kind, to define a mathematical model for the craniometric dimensions of the posterior ventricular entry point and also the corresponding trajectory in reference to external auditory meatus in pediatric patients. The model used the patient’s sex and age. Our validation result has proven our model to be highly successful with low error and acceptable parenchymal mantle.
Various methods have been tried to insert the catheter in a location that would be free-floating in the ventricular space, including stereotactic placement of the catheter or use of stereotactic technology to define the entry point and trajectory, use of endoscope, and use of variety of devices for advancement of the catheter in the appropriate trajectory [10-13]. The thought of placement of ventricular catheter without the use of such sophisticated technology may be of use for young neurosurgeons who do not have the spatial orientation to puncture the ventricles from the posterior of the skull. Also, the utility of such a point and trajectory in ventricular catheterization of patients with slit ventricle syndrome cannot be over-emphasized.
Supposing that the best posterior ventricular catheter is the one with the least traversing brain parenchyma, with its tip residing in the posterior horn, there would be an infinite series of initial burr holes and trajectories and catheter length. Considering one or two of these variables constant, the number of options would be much narrowed. In our previous report, we tried to keep the entry plane and trajectory constant, thus, we could find the initial burr hole place. In this report, we used the same method to find the burr hole place [8].
The reference point in all previously proposed posterior entry points was inion [14]. Inion, the tip of the external occipital protuberance, is usually an easy-to-find bony landmark to be used as a reference point. Besides the occasions of not being palpable, inion may not be the exact external equivalent for internal occipital protuberance, the torcular herophili, or the interception of the tentorial plate and falx. Therefore, using inion as the reference point may fool the surgeon in order to find the precise posterior entry points [15]. We have used the external auditory meatus in our previous report. We demonstrated that the coefficient of variation for craniometrics dimensions of entry point using external auditory meatus as the reference point was less than that of entry point using inion as the reference point. Thus, the external auditory meatus was used as the reference point in this study [15]
Historically, there are three points by which the ventricles can be cannulated from the posterior of the skull, i.e., Keen, Dandy, and Frazier points. Morone et al. have published a review on these points regarding their burr hole place and their trajectory [14]. Cheng et al. have tried to gain access to the atrium from the occipital horn, which may not be acceptable in the shunt procedure, although it may be of use in endoscopic surgery [16]. Others have tried to cannulate the temporal horn through the occipital horn, which again is not the case for the shunt surgery [17].
According to Lind et al., there is a wide range of burr holes and reference points used by neurosurgeons for posterior approaches in shunt placement [18]. Multiple authors have tried to define entry points for ventricular access from the posterior skull; yet, none of them has been validated or evaluated in pediatric patients. Moreover, none of the studies have geometrically proved that the trajectory has traversed the least brain parenchyma. For instance, Duong et al. have chosen a point in the posterior atrial wall in an axial CT scan slice, by which, as they speculate, put the least brain thickness in hazard, although was not proven and validated [19]. Other proposed points are presented in detail in Table 4.
Our result showed that the geometric position of the entry point compared to the reference point is defined by age and sex, but not the head circumference. This is in contrast to the expectation that head circumference and age are correlated both physiologically and statistically. We do not have a good explanation, but a postulation could be that although the two quantities are statistically correlated in our specimen, age is a much more varied quantity rather than head circumference, as its coefficient of variation is more than that of head circumference.
Finally, one of the positive points of our study is the model validation step. As mentioned, none of the previously proposed points has been validated, making them not reliable for general use. Validation of our model found a high success rate for entering the ventricle, and also the path traveled in the brain did not differ between the main and validation groups. These results show that our model is usable and can accurately determine the appropriate path to enter the ventricle through posterior approach.
Limitations
Children with subclinical skull deformity were not excluded from the samples. As the most common skull deformity in children is sagittal craniosynostosis, the subclinical forms of this disease are common. We did not evaluate the cranial index to stratify the patients according to the severity of sagittal craniosynostosis. The model needs to be verified in another set of patients with and without hydrocephalus. Moreover, we did not study the patients with hydrocephalus, in whom the entry point, and/or catheter trajectory may be different. Using the same plane in axial CT images, the shape of the lateral ventricles is not the same in different people. We could not compensate for this issue in the current study.
Conclusion
We have developed a mathematical model to define a posterior entry point for ventricular catheterization in children according to age and sex, which injures the least brain parenchyma to reach the ventricle. Our model has shown promising results on validation and we believe it provides valuable insights for pediatric neurosurgeons who are looking for ways to improve the success rate of ventricular catheter placement and shunt survival in pediatric patients.
Declarations
Statement of ethics: This study was approved by the ethical council of Tehran University of Medical Science (IR.TUMS.MEDICINE.REC.1398.654).
Conflict of interest statement: The authors have no conflicts of interest to declare.
Funding sources: This study was not supported by any sponsor or funder.
Author contributions: Literature review: KTM; Data Analysis: SFM, MADO, AI; Manuscript Writing: SFM, MADO, AJ, KTM; Manuscript Revision: MEK, ZH, FN, KTM; Data Collection: SFM, HE, HD, AI, MRKD
Funding statement: This study was not supported by any sponsor or funder
Data availability statement: All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
References
- Eide PK, Lundar T. Arne Torkildsen and the ventriculocisternal shunt: the first clinically successful shunt for hydrocephalus. J Neurosurg. 2016; 124(5): 1421-8. doi: 10.3171/2015.1.Jns142659
- Dewan MC, Lim J, Shannon CN, Wellons JC. The durability of endoscopic third ventriculostomy and ventriculoperitoneal shunts in children with hydrocephalus following posterior fossa tumor resection: a systematic review and time-to-failure analysis. Journal of Neurosurgery: Pediatrics. 2017; 19(5): 578-584. doi: 10.3171/2017.1.PEDS16536
- Hanak BW, Bonow RH, Harris CA, Browd SR. Cerebrospinal Fluid Shunting Complications in Children. Pediatric neurosurgery. 2017; 52(6): 381-400. doi: 10.1159/000452840
- Jorgensen J, Williams C, Sarang-Sieminski A. Hydrocephalus and Ventriculoperitoneal Shunts: Modes of Failure and Opportunities for Improvement. Critical reviews in biomedical engineering. 2016; 44(1-2): 91-7. doi: 10.1615/CritRevBiomedEng.2016017149
- Collins P, Hockley AD, Woollam DH. Surface ultrastructure of tissues occluding ventricular catheters. J Neurosurg. 1978; 48(4): 609-13. doi: 10.3171/jns.1978.48.4.0609
- Kingsly EN, Kanumba ES, Lemeri L. Outcome Of Ventriculo-Peritoneal Shunts Inserted At The Parieto-Occipital Area: A One-Year Experience At Muhimbili Orthopaedic Institute, Dar Es Salaam. [Dissertation]. 2012.
- Keen WW. Surgery of the lateral ventricles of the brain. The Lancet. 1890; 136(3498): 553-555. doi: 10.1016/S0140-6736(00)48676-9.
- Tayebi Meybodi K, Hoseinzadeh E, Ahmadi M, Taghvaei M, Saberi H. Reevaluation of Classic Posterior Ventricular Puncture Sites Using a 3-Dimensional Brain Simulation Model. World neurosurgery. 2017; 107: 22-27. doi: 10.1016/j.wneu.2017.07.134
- Zhang Z. Variable selection with stepwise and best subset approaches. Annals of translational medicine. 2016; 4(7): 136. doi: 10.21037/atm.2016.03.35
- Wilson TJ, Stetler WR, Al-Holou WN, Sullivan SE. Comparison of the accuracy of ventricular catheter placement using freehand placement, ultrasonic guidance, and stereotactic neuronavigation. J Neurosurg. 2013; 119(1): 66-70. doi: 10.3171/2012.11.Jns111384
- Azeem SS, Origitano TC. Ventricular catheter placement with a frameless neuronavigational system: A 1-year experience. Neurosurgery. 2007; 60(4 Suppl 2): 247-8. doi: 10.1227/01.Neu.0000255387.03088.53
- Chandler WF, Knake JE, McGillicuddy JE, Lillehei KO, Silver TM. Intraoperative use of real-time ultrasonography in neurosurgery. J Neurosurg. 1982; 57(2): 157-63. doi: 10.3171/jns.1982.57.2.0157
- Huyette DR, Turnbow BJ, Kaufman C, Vaslow DF, Whiting BB, et al. Accuracy of the freehand pass technique for ventriculostomy catheter placement: retrospective assessment using computed tomography scans. J Neurosurg. 2008; 108(1): 88-91. doi: 10.3171/jns/2008/108/01/0088
- Morone PJ, Dewan MC, Zuckerman SL, Tubbs RS, Singer RJ. Craniometrics and Ventricular Access: A Review of Kocher’s, Kaufman’s, Paine’s, Menovksy’s, Tubbs’, Keen’s, Frazier’s, Dandy’s, and Sanchez’s Points. Operative neurosurgery (Hagerstown, Md). 2020; 18(5): 461-469. doi: 10.1093/ons/opz194
- Tubbs RS, Salter G, Oakes WJ. Superficial surgical landmarks for the transverse sinus and torcular herophili. J Neurosurg. 2000; 93(2): 279-81. doi: 10.3171/jns.2000.93.2.0279
- Cheng S, Dong Y, Han C, Tong D. Morphometric study of endoscopic transoccipital approach to lateral ventricle with magnetic resonance imaging. J Craniofac Surg. 2016; 27(7): e716-718. doi: 10.1097/SCS.0000000000001820
- Sánchez JJ, Rincon-Torroella J, Prats-Galino A, de Notaris M, Berenguer J, et al. New endoscopic route to the temporal horn of the lateral ventricle: surgical simulation and morphometric assessment. J Neurosurg. 2014; 121(3): 751-9. doi: 10.3171/2014.5.Jns132309
- Lind CR, Tsai AM, Law AJ, Lau H, Muthiah K. Ventricular catheter trajectories from traditional shunt approaches: A morphometric study in adults with hydrocephalus. J Neurosurg. 2008; 108(5): 930-3. doi: 10.3171/jns/2008/108/5/0930
- Duong J, Elia CJ, Miulli D, Dong F, Sumida A. An approach using the occipital parietal point for placement of ventriculoperitoneal catheters in adults. Surgical neurology international. 2019; 10: 21. doi: 10.4103/sni.sni_3_18