Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Luca Cioccari1,2*; David Berger1,3
*Corresponding Author: Luca Cioccari
Department of Intensive Care Medicine, Kantonsspital Aarau, Tellstrasse 25 CH-5001 Aarau, Switzerland.
Email: luca.cioccari@ksa.ch
Article Info
Received: Nov 04, 2024
Accepted: Dec 02, 2024
Published: Dec 09, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Cioccari L (2024).
Abstract...
Respiratory variations in the diameter of the superior and inferior vena cava are commonly used to assess intravascular volume status and predict fluid responsiveness in critically ill patients. However, these variations may be unreliable in conditions affecting intrathoracic and intra-abdominal pressures. We present a case of a 65-year-old man with severe acute respiratory distress syndrome who developed intra-abdominal hypertension due to intestinal ischemia, resulting in differential collapsibility of the inferior and superior vena cava. This finding reinforces the need for cautious interpretation of vena cava measurements in abdominal compartment syndrome, as these measurements may not accurately reflect volume status or fluid responsiveness in these patients.
Keywords: Abdominal compartment syndrome; ARDS; Vena cava; Echocardiography.
Citation: Cioccari L, Berger D. Differential Collapsibility of the Vena Cava in Abdominal Compartment Ayndrome - A Case Report. J Clin Med Surgery. 2024; 4(2): 1176.
Introduction
Respiratory variations in the diameter of the superior and inferior vena cava have been used to assess intravascular volume status and fluid responsiveness in surgical, medical, and critically ill patients [1-3]. However, the collapsibility or distensibility of the vena cava is affected by various conditions leading to variations in intrathoracic and intra-abdominal pressure [4]. In such circumstances, respiratory variations in the diameter of the superior and inferior vena cava can be misleading [5]. We present a case of differential collapsibility of the vena cave in the setting of intra-abdominal hypertension.
Case presentation
A 65-year-old overweight man was admitted to the ICU and intubated for severe acute respiratory distress syndrome. Ten days after ICU admission, he developed intra-abdominal hypertension with an intra-abdominal pressure of 22 mmHg due to intestinal ischaemia. The clinical course was complicated by haemodynamic shock, acute renal failure and deteriorating respiratory compliance. He was treated with 20 ml/kg crystalloids and high doses of vasopressors were given for catastrophic haemodynamic collapse. Transthoracic echocardiography showed an Inferior Vena Cava (IVC) diameter of 2 cm without respiratory variation (Figure 1). Simultaneous transesophageal echocardiography showed hyperdynamic systolic LV function with kissing ventricles and a 22% collapsibility of the superior vena cava (Figure 2) while the patient was on volume-controlled ventilation with an end-expiratory positive pressure of 16 cm H2O and a plateau pressure of 34 cm H2O. Immediate laparotomy and right-sided hemicolectomy were performed, followed by open-abdomen treatment. However, the patient deteriorated rapidly and died a few hours later of refractory septic shock and multiorgan failure.
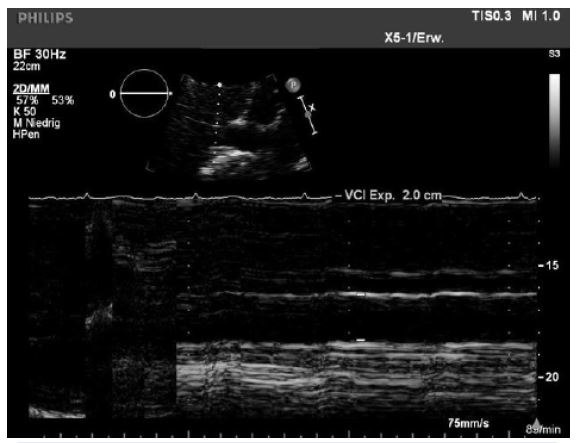
Figure 1: Transthoracic Echocardiography (TTE) image of the inferior vena cava measuring 2 cm without respiratory variations in diameter.

Figure 2: Transesophageal Echocardiography (TEE) image of the superior vena cave with visible respiratory variations in diameter (22% collapsibility).
Discussion
Differential collapsibility of the vena cava is the echocardiographic manifestation of increased intra-abdominal venous pressure and consequent decreased thoracic venous return in patients with abdominal compartment syndrome. The SVC collapsibility index in our case did not reach the proposed threshold of 36% for fluid responsiveness [2]. However, the TEE was performed after at least 20 ml/kg of crystalloids and high doses of vasopressors had been administered for catastrophic haemodynamic collapse. In addition, the patient was mechanically ventilated with higher than normally recommended airway pressures due to poor respiratory compliance. Nevertheless, the discrepancy between the respiratory variations of the IVC and SVC was still apparent and illustrates well why IVC collapsibility cannot be used to assess volume responsiveness in situations of increased abdominal pressure.
Conclusion
Respiratory variations in vena cava diameter are influenced by variations in both intrathoracic and intra-abdominal pressure. Our case highlights the fact that they are unreliable indicators of fluid responsiveness in patients with abdominal compartment syndrome.
Declarations
Conflicts of interest: LC has received research grants from the University of Bern, the Inselspital Bern and the research coucil of the Cantonal Hospital Aarau, as well as educational grants from Hamilton Medical and Fresenius Medical Care and speaker honoraria from OrphaSwiss. None are related to this work.
Funding statement: Not applicable.
Ethics approval and consent for publication: All information and images presented are anonymized and, therefore, do not require ethics approval or consent for publication.
References
- Barbier C, Loubières Y, Schmit C, Hayon J, et al. Respiratory changes in inferior vena cava diameter are helpful in predicting fluid responsiveness in ventilated septic patients. Intensive Care Med. 2004; 30(9): 1740-1746.
- Vieillard-Baron A, Chergui K, Rabiller A, Peyrouset O, et al. Superior vena caval collapsibility as a gauge of volume status in ventilated septic patients. Intensive Care Med. 2004; 30(9): 1734-1739.
- Feissel M, Michard F, Faller JP, Teboul JL. The respiratory variation in inferior vena cava diameter as a guide to fluid therapy. Intensive Care Med. 2004; 30(9): 1834-1837.
- Bauman Z, Coba V, Gassner M, Amponsah D, et al. Inferior vena cava collapsibility loses correlation with internal jugular vein collapsibility during increased thoracic or intra-abdominal pressure. J Ultrasound. 2015; 18(4): 343-348.
- Bodson L, Vieillard-Baron A. Respiratory variation in inferior vena cava diameter: Surrogate of central venous pressure or parameter of fluid responsiveness? Let the physiology reply. Crit Care. 2012; 16(6): 181.