Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Hodkiewicz Victoria A1*; Siemers Parinaz J2; Di Chiaro Bianca2; Kujalowicz Christopher1; King Timothy W2,3
*Corresponding Author: Victoria Hodkiewicz A
Department of Surgery, Division of Plastic and Reconstructive Surgery, Loyola University Stritch School of Medicine, Maywood, IL, USA.
Tel: 262-903-1001;
Email: vhodkiewicz@luc.edu
Article Info
Received: Oct 29, 2024
Accepted: Nov 28, 2024
Published: Dec 05, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Victoria HA (2024).
Abstract...
We present a modified surgical technique to improve both sexual and aesthetic outcomes for a patient undergoing oncologic Abdominoperineal Resection (APR) followed by Vertical Rectus Abdominis Myocutaneous (VRAM) flap reconstruction. Here, we describe a surgical technique involving deepithelialization and skin bridge formation.
Keywords: VRAM flap; Abdominoperineal resection; Reconstructive surgery; Surgical technique; DE epithelialization; Perineal reconstruction; Rectal cancer.
Citation: Victoria HA, Parinaz SJ, Bianca DC, Christopher K, Timothy KW. Depithelialization of VRAM Skin Bridge for Perineal Reconstruction: Modified Technique. J Clin Med Surgery. 2024; 4(2): 1175.
Introduction
Abdominoperineal Resection (APR) is the curative or palliative resection of pelvic cancer including the involved urinary, reproductive and/or hindgut visceral structures, but leaves a large surgical defect in a challenging anatomic location in patients who oftentimes have surrounding irradiated tissue and/or poor immune status [1-3]. High rates of surgical-site morbidity following APR poses a reconstructive challenge to plastic surgeons [4]. Surgical defects may be repaired with primary closure, secondary closure or flap-based reconstruction (most commonly the rectus abdominis, myocutaneous, gracilis, or gluteal flap) [5], and the selection of which modality is a topic of debate across the literature. Some studies have indicated that even when primary closure is feasible, flap reconstruction may be the preferred reconstructive option due to decreased total perineal wound complications [6,7].
The Vertical Rectus Abdominis Myocutaneous (VRAM) flap is a well-known flap in the plastic surgeon’s armamentarium, and is often the flap of choice by plastic surgeons for reconstruction following APR. This flap is particularly useful for reconstruction of the posterior vaginal wall due to its cutaneous paddle which aids in the creation of the vaginal lining, bulk for obliteration of dead space, and the flap’s reliable vascularity [8]. In comparison to the gluteal and gracilis flaps, studies suggest that the VRAM flap has significantly lower wound or flap complications [9].
Here, we describe the use of a modified technique of the VRAM flap for perineal reconstruction that includes De epithelization and formation of a skin bridge to best recontrust the native perineal surface anatomy.
Case report
A 62 year-old female with history of primary rectal adenocarcinoma status post Lower Anterior Resection (LAR), Diverting Loop Ostomy (DLI), and chemoradiation six years prior, now presented with new-found metastasis involving the sacrum, uterus, and posterior vaginal wall. After review of the patient’s current oncological status and thorough discussion of goals of care with the patient, surgical resection and reconstruction performed. The multidisciplinary surgical procedure includes efforts from General Surgery (Abdominal Perineal Resection (APR) with end-colostomy and small bowel resection; Intraoperative radiation therapy), Obstetrics & Gynecology Surgery (Open Total Hysterectomy (TAH), Bilateral Salpingo-Oophorectomy (BSO), posterior vaginectomy), and Plastic & Reconstructive Surgery (Myocutaneous Flap (VRAM) for Vaginal and APR reconstruction). A modified technique of the VRAM for Vaginal and APR reconstruction was utilized, as described below.
Surgical technique
The patient was placed in a lithotomy position. APR with end-colostomy and small bowel resection (with intraoperative radiation therapy), TAH-BSO, and posterior vaginectomy were performed. Due to the patient’s previous right-sided ostomy site, we used a left VRAM flap for reconstruction.
The VRAM flap was premeasured to reconstruct the posterior vaginal wall and perineum. The patient previously had a laparotomy with an incision around the right side of the umbilicus, therefore, the same incision was used. Identification of the posterior vertical rectus abdominis and separation from the peritoneal lining was performed.
Separation was continued until the arcuate line was reached. The posterior fascia was elevated off the entire posterior muscle superiorly. Attention was then turned to the anterior muscle dissection. First, the subcutaneous fat was separated from the rectus abdominis muscle superiorly and inferiorly. The muscle was elevated off the fascia moving superiorly until reaching the tendinous inscription. The muscle was freed from the inscription all the way to the lateral edge. Color doppler ultrasonography was utilized to identify multiple perforators. Further anterior fascia dissection proceeded, taking care not to avulse the identified perforators. The dissection continued until the remaining inscriptions were reached. To free the additional inscription from the underlying muscle, the same process as described above was repeated until the superior edge of the muscle was reached. At this point, the superior edge of the vertical rectus abdominis muscle was clamped and divided.
Attention was turned to the pre-measured surface for vaginal and perineal reconstruction. A skin incision was extended around the pre-measured area, and dissection through the subcutaneous fat proceeded until only the muscle and subcutaneous tissue (preserved based off of the perforators) remained. Indocyanine green dye was injected for the SPY machine sterilely. It was then flushed with 10 mL of normal saline. The SPY machine was then employed to ensure that all areas of harvested flap were viable. Areas that were nonviable were marked and excised accordingly.
The VRAM flap was now ready for transfer. It was carefully rotated and delivered through the opening of the vagina and perineal area. Moving down to the lithotomy position, the previous packing was removed and then from the vaginal opening, the flap was inset using 2-0 Vicryls. This was accomplished distally first, and then along both vaginal mucosal edges until reaching the introitus.
Modified surgical technique
Standard prior techniques would continue sutures to create a linear, continuous vaginal, perineal, and rectal flap without anterior and posterior distinction. To better emulate native female anatomy with vaginal and anal area separation, our surgeon’s modified technique constructs a skin bridge to mimic these anatomic distinctions. The introitus location is marked on the VRAM flap, and then two triangles are DE epithelialized with their points meeting where the skin bridge will later be sutured over (Figure 1). Care is taken to avoid the flap’s perforators. The introitus is closed at the meeting point of the two deepithelialized triangles. Once the vaginal introitus is formed, inset of the mucosa at the vagina and then the perineum is performed. The remaining perineal flap is inset while excess flap is deepithelialized and then tucked into the perineum. The rest of the perineum is closed (Figure 2).
Vertical Rectus Abdominis Myocutaneous (VRAM) flap showed good perfusion at one month and one year follow-up (Figures 3 and 4) and the patient had no intraoperative or postoperative complications. Deepithelialization of the skin bridge at the perineal border allowed for better inset of the VRAM flap with a better aesthetic and functional long-term outcomes.
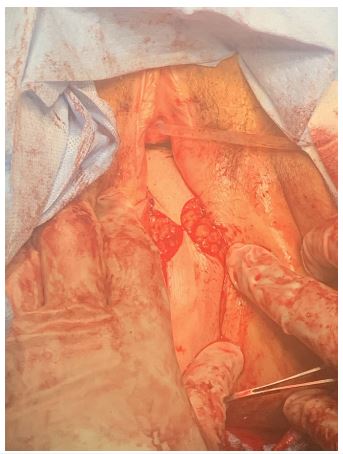
Figure 1: Deepithelialization of VRAM flap prior to closure.

Figure 2: Perioperative results following closure of skin bridge.

Figure 3: Postoperative results at one month.

Figure 4: Postoperative results at one year.
Discussion
Free flap tissue transfer is the standard for soft tissue reconstruction following many oncological resection procedures [10]. Specifically, the Vertical Rectus Abdominis Myocutaneous flap (VRAM) is commonly utilized for primary closure of large perineal defects, as it serves as a well-vascularized tissue which may contribute to reduced perineal wound complications following chemoradiotherapy without increasing abdominal wall complications [3]. With that being said, perineal flap morbidity rates remain high as demonstrated by Radwan et al. [11], states, “mean perineal flap morbidity was 27%, with a complete flap loss rate of 1.8% and a perineal hernia rate of 0.2%. Mean donor site morbidity was 15%, with an abdominal dehiscence rate of 5.5% and an incisional hernia rate of 3.3%.” Overall, although flap morbidity is significant, major complication risks remain low. Despite the risks in such patients requiring radical surgical resection due to progressive metastasis, the VRAM flap is commonly preferred by plastic surgeons as it offers the ability to modify flap design while maintaining proper vascularization throughout oncological treatments.
Although frequently used for such defects, the traditional VRAM technique for perineal reconstruction leaves patients with an undesirable external appearance. Not only does this have a profound impact on patients’ self-image, but adds additional distress as it limits patients’ sexual function post-operatively. The standard reconstructive technique leaves patients with a distorted body image due to the suboptimal flattened shape and lack of anterior and posterior separation. Our case illustrates how the addition of a minor step adds significant value to a patients’ aesthetic and functional outcomes. DE epithelialization of two triangles along the VRAM flap to then form a closed skin bridge creates a separation with defined anal and urogenital triangles. Emulating native female anatomy following major oncological resections has a profound impact on patients’ self-image and should be a plastic and reconstructive surgeon’s priority while performing such operations.
It is critical to manage each case based on patients’ cosmetic and sexual goals. Variables may apply such as stage of metastasis and magnitude of oncological resection, comorbidities, and risk for infection. Although these should be accounted for and thoroughly discussed with each patient to best restore various forms of resections, we suggest that this minor modification be implemented in all applicable VRAM perineal reconstruction candidates. This new surgical technique adds significant value to the patient’s overall surgical result, psychological well being, and improves upon sexual functionality following major oncologic resections.
Conclusion
The key to successful APR utilizing the VRAM flap is to best emulate native surface anatomy. We believe that the utilization of our modified technique involving DE epithelization and formation of a skin bridge should be applied to similar patient cases, and offers a significant improvement to patient satisfaction.
Declarations
Conflicts of interest: The authors report there are no competing interests to declare. The authors alone are responsible for the content and writing of the paper.
Funding: No funding was received for this article.
References
- Kreutz-Rodrigues L, Banuelos J, Saleem HY, Mills AM, Tran NV, et al. The Use of Vertical Rectus Abdominis Myocutaneous Flap for Pelvic Reconstruction: What Are the Risk Factors for Complications? Plast Reconstr Surg Glob Open. 2019; 7(8 Suppl): 75-75.
- Perry WB, Connaughton JC. Abdominoperineal resection how is it done and what are the results? Clin Colon Rectal Surg. 2007; 20(3): 213-220.
- Butler CE, Gündeslioglu AO, Rodriguez-Bigas MA. Outcomes of immediate vertical rectus abdominis myocutaneous flap reconstruction for irradiated abdominoperineal resection defects. J Am Coll Surg. 2008; 206(4): 694-703. doi: 10.1016/j.jamcollsurg.2007.12.007.
- Devulapalli C, Jia Wei AT, DiBiagio JR, Baez ML, Baltodano PA, et al. Primary versus Flap Closure of Perineal Defects following Oncologic Resection: A Systematic Review and Meta-Analysis. Plast Reconstr Surg. 2016; 137(5): 1602-1613. doi: 10.1097/PRS.0000000000002107.
- Copeland-Halperin LR, Stewart T, Chen Y, Funderburk CD, Freed GL. Perineal reconstruction following abdominoperineal resection: Comprehensive review of the literature. J Plast Reconstr Aesthet Surg. 2020; 73(11): 1924-1932. doi: 10.1016/j.bjps.2020.08.090.
- Temperley HC, Shokuhi P, O’Sullivan NJ, Mac Curtain B, Waters C, et al. Primary closure versus vertical rectus abdominis myocutaneous (VRAM) flap closure of perineal wound following abdominoperineal resection-a systematic review and meta-analysis. Ir J Med Sci. 2024; 193(4): 1721-1728. doi: 10.1007/s11845-024-03651-3.
- Yang XY, Wei MT, Yang XT, He YZ, Hao Y, et al. Primary vs myocutaneous flap closure of perineal defects following abdominoperineal resection for colorectal disease: A systematic review and meta-analysis. Colorectal Dis. 2019; 21(2): 138-155. doi: 10.1111/codi.14471.
- Campbell, et al. Use of adjuvant techniques improves surgical outcomes of complex VRAM flap reconstructions of pelvic cancer defects. Plast Reconstr Surg. 2011; 128(2): 447-458.
- Johnstone MS. Vertical Rectus Abdominis Myocutaneous versus Alternative Flaps for Perineal Repair after Abdominoperineal Excision of the Rectum in the Era of Laparoscopic Surgery. Ann Plast Surg. 2017; 79(1): 101-106. doi: 10.1097/SAP.0000000000001137.
- Shervin Zoghi, Kelsey Millar, Steven Thorpe, Christopher O. Bayne. Late lower extremity free flap vascular compromise and salvage in a Pediatric patient diagnosed with monophasic synovial sarcoma, Case Reports in Plastic Surgery and Hand Surgery. 2023; 10: 1.
- Radwan RW, Tang AM, Harries RL, Davies EG, Drew P, et al. Vertical rectus abdominis flap (VRAM) for perineal reconstruction following pelvic surgery: A systematic review. J Plast Reconstr Aesthet Surg. 2021; 74(3): 523-529. doi: 10.1016/j.bjps.2020.10.100.
- D’Souza, et al. Vaginal Reconstruction Following Resection of Primary Locally Advanced and Recurrent Colorectal Malignancies. Arch Surg. 2003; 138(12): 1340-1343.
- Berger, et al. Modified VRAM flap vaginal reconstruction: an analysis of surgical outcomes. Gynecol Oncol. 2012; 125(1): 252-5.
- Rouch JD, Li A, Cohen JG, Kazanjian KK, Festekjian JH. Re-exploration of vertical rectus abdominis myocutaneous flap for vaginal reconstruction: Case report and review of the literature. JPRAS Open. 2017; 15: 32-35.
- Gabrielle A La Bove, Gregory RD Evans, Brian Biggerstaff, Brandon K Richland, Seung Ah Lee, et al. Ten-Year experience with vertical rectus abdominis myocutaneous flap for reconstruction of abdominoperineal resection defects. JPRAS Open. 2021; 27: 90-98.
- Rouch JD, Li A, Cohen JG, Kazanjian KK, Festekjian JH. Re-exploration of vertical rectus abdominis myocutaneous flap for vaginal reconstruction: Case report and review of the literature. JPRAS Open. 2017; 15: 32-35.