Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Tayeh S*; Subramonian S; Denoiseux C; Parvanta L
*Corresponding Author: Tayeh S
Senior Clinical Fellow in General and Breast Surgery, Homerton University Hospital Foundation Trust, Homerton Row, London E9 6SR, UK.
Email: salim.tayeh@nhs.net
Article Info
Received: Oct 03, 2024
Accepted: Nov 18, 2024
Published: Nov 25, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Tayeh S (2022).
Abstract...
Introduction: Wire-Guided Localisation (WGL) is the most widely used technique for surgical excision of non-palpable breast lesions. However this method has limitations including wire transection/migration and inflexible scheduling. To combat this, recent technological advances have created wireless, radiation-free localization methods, like the LOCalizer™, based on Radio-Frequency Identification (RFID) technology. In this prospective study, we evaluated the role of RFID and compared it to WGL in our District General hospital.
Methods: We prospectively evaluated 10 cases of RFID as a clinical evaluation of this technique. We compared the results to the wire guided cases done during the same study period (from November 2021 to September 2022).
The evaluation focused on:
· Successful localizations.
· Identification and retrieval.
· Status of surgical margins, need for re-operation.
· Resected specimen weight.
Results: 10 RFID tags (6 malignant, 4 benign cases) were deployed under Ultrasound guidance, and 24 wires were deployed (20 cancer, 4 benign cases) under Ultrasound or Mammogram guidance, to localize non-palpable breast lesions. All tags and wires (except 1 wire case) were deployed and localized successfully, and all target lesions were retrieved successfully.
The average number of days between tag/wire insertion and surgery was 0 for wires, and 18.9 (6-55) days for tags. The reoperation rate for positive margins was 30% (6/20) for wires and 16.7% (1/6) for tags. The average number of shaves taken per case was 2 for wires, and 1.5 for tags. The average specimen weight (for cancer cases only) was 51g for wires, and 57g for tags.
Conclusion: Our study demonstrates that radiofrequency localization technology is an effective and comparable alternative to wire-guided localization, with the added advantage of decoupling surgery and radiology scheduling.
Keywords: Non palpable breast cancer; Localization; Wireless device; Radiofrequency device; Surgical margins.
Citation: Tayeh S, Subramonian S, Denoiseux C, Parvanta L. Wires or Tags? Localizing Non-Palpable Breast Lesions in a District General Hospital. J Clin Med Surgery. 2023; 4(2): 1174.
Introduction
Breast cancer is common, forming 11.7% of all cancers diagnosed globally in 2020 [1], making it the most common cancer worldwide. There has also been an increase in non-palpable breast cancers/lesions due to the national UK mammographic screening programme and the use of neoadjuvant chemotherapy, resulting in down-sizing of the palpable tumors. Non palpable lesions are often small, occult lesions that are amenable to Breast Conserving Surgery (BCS). These non-palpable lesions need to be localized before surgery in order to aid surgical removal.
Wire Guided Localization (WGL) has been the gold standard for localizing non-palpable breast lesions since the 70s [2], and involves the insertion of a hook into the lesion (under radiological guidance) which is connected to a wire through the skin. However this method has limitations; it can be painful for the patient, and introduce a possible risk of sharps injury to the surgeon. Furthermore, logistical difficulties in scheduling wire insertion mean wires need to be inserted on the same day as surgery, causing additional anxiety for the patient and scheduling difficulties for the operating team. There is also a risk of wire migration, which can reduce the chance of successful lesion localization, and possible need for re-operation in the future.
Thus alternative techniques have been developed for localization of non-palpable lesions. Examples of these techniques are: Radiofrequency ID tags (RFID), SAVI SCOUT and Magseed.
In this study, we have examined the performance of a wireless localization technology that uses glass-enclosed Radio Frequency Identification (RFID) tags, LOCalizerTM, and compared it to wire-guided localization.
Material and methods
Female patients aged 18 years or older with nonpalpable breast lesions necessitating surgical excision were enrolled in this observational clinical evaluation conducted at Homerton Hospital (London, UK). The study spanned from November 2021 to September 2022. A total of 10 patients were recruited for the RFID arm of the study, while 24 patients underwent Wire-Guided Localisation (WGL) during the same period. The indications for surgery included non-palpable malignancy, malignant lesions rendered non-palpable post Neoadjuvant Chemotherapy (NACT), and pathologically intermediate (B3) nonpalpable lesions requiring diagnostic surgical excision. All participants provided informed consent, and the use of RFID technology was approved by the institutional review board.
For the RFID arm of the study, the Localizer (Hologic) RFID system was utilized. Image-guided deployment of RFID tags was performed up to 60 days prior to surgery. Under image guidance, RFID tags were percutaneously inserted into the breast tissue through a delivery needle. Post-procedure mammography was employed to confirm the position of the RFID tags. Surgery was conducted within the designated timeframe following tag deployment. The tags and wires were deployed and retrieved by the same radiology and surgery teams.
The primary endpoint of this study was to evaluate the extent of successful RFID tag deployment and retrieval. Secondary endpoints included assessing radial surgical margins, the need for re-operation, specimen weight, and the number of shaves for malignant cases. Additionally, logistical ease was measured by recording the number of days between RFID tag insertion and the date of surgery.
Results
10 RFID tags (6 malignant, 4 benign cases) were deployed under Ultrasound guidance, and 24 wires were deployed (20 cancer, 4 benign cases) under Ultrasound or Mammogram guidance, to localize non-palpable breast lesions. All tags and wires (except 1 wire case) were deployed and localized successfully, and all target lesions were retrieved successfully.
Table 1 demonstrates our results as shown for wires and tags. As shown, the average number of days between wire insertion and surgery was zero (as the preop insertion of the wire had to be done near to surgery to avoid wire migration/displacement). However, the average number of days between tag insertion and surgery was 18.9 days (ranging from 6 to 55). Thus tags can be inserted completely separately to the date of surgery, allowing for greater flexibility in preoperative scheduling. The reoperation rate for positive margins for wires was 30%, compared to 16.7% for tags. The average number of shaves for wire cases was 2, whereas it was 1.5 for tag cases. Finally, the average specimen weight for wire cases was 51g, compared to 57g for tag cases.
Table 1: Comparison between wires and tags.
| Wires | Tags | |
|---|---|---|
| Total number of breast lesions | 24 | 10 |
| Number of benign lesions | 4 | 4 |
| Number of malignant lesions | 20 | 6 |
| The average number of days between tag/wire insertion and surgery | 0 | 19 days(6-55 range) |
| Reoperation rate for positivemargins | 6/20 (30%) | 1/6 (16.7%) |
| Average numbershaves formalignant cases | 2 (Range 0-5) | 1.5 (Range0-5) |
| The average distance between the wire/tag and the marker/lesion(for all cases benign andcancer) | 7.1 mm(Range 0-17) | 3.1 mm(Range 0-11) |
| Average specimen weight (Onlycancer cases) | 51g(range 3.5-235 g) | 57g(Range 28.2-129 g) |
| Successful retrieval of the wire/tags | 100% | 100% |
| Successful insertion rate | 23/24 (95.8%)(In one case, the wire was inserted 24 mm away from the marker,prompt- ing theinsertion of another wire). | 100% |
A chi-squared test was performed to compare the ‘Reopera- tion rate’ for wires and tags, which did NOT demonstrate a sig- nificant difference (p=0.51).
Discussion
Wire guided localization has been the standard technique in localizing breast lesions for decades. Wire guided localization involves the insertion of a wire into the breast with radiological skin markings. The advantage of wire guided localization is that the majority of breast surgeons across the world are well experienced in this technique and it has been the standardized technique across the world for many years, with a vast range of research published on its uses and outcomes. It is an inexpensive localization method and does not require any special radiofrequency or magnetic equipment, thus also allowing its use in patients with pacemakers or cardiac devices. However, wire insertion and surgery need to be done on the same day, which causes difficulties when surgeries are rescheduled. The wire is uncomfortable for patients and poses a risk of needle stick injury to surgeons. Furthermore, there is a risk of wire migration [3], leading to inaccurate lesion localization.
In order to overcome the challenges created by wire guided localization, a number of wire-free technologies have been trialled. We have discussed 3 methods: Radiofrequency ID tags (RFID), SAVI SCOUT and Magseed.
Radiofrequency ID (RFID) devices offer a wire-free approach to non-palpable lesion localization [4]. A Radiofrequency ID tag with a unique ID number is deployed into the breast using a 12 G introducer. A handheld surgical probe detects the RFID tag and displays the distance to the tag in millimetres as well as the tag’s unique ID number. This technique is illustrated in Figure 1 below. The LOCalizerTM is able to accurately and quickly estimate the distance from the probe to the tag, enabling for a precise excision, but this range is limited to 6cm, which is problematic in larger breasts or deeper lesions. The RFID tags also cause artefact on MRI scans, and patients with cardiac pacemakers and defibrillators are excluded from RFID tag insertion as the radiofrequency field may interfere with the functioning of these devices.However, more data is needed on the long-term outcomes of these RFID devices as the long-term implications of these non-wire devices are not well understood.

Figure 1: Comparison between wires and tags.
Figures 2 and 3 demonstrate the appearance of RFID tag on mammogram (Figure 2) and on Xray (Figure 3).
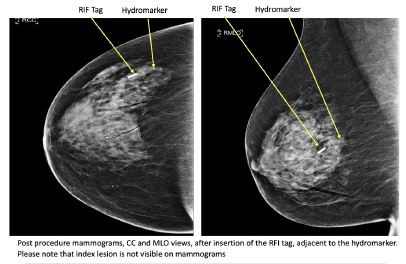
Figure 2: RFID tags in situ on post-procedure mammogram Image on the left-Craniocaudal Mammogram showing RFID tag Image on the right- MLO Mammogram view showing RFID tag.
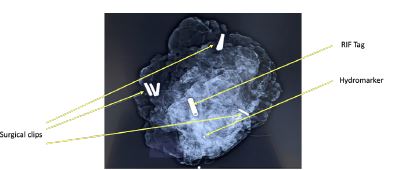
Figure 3: Appearance of RFID tag on Xray, noted lesion not seen on this x-ray.
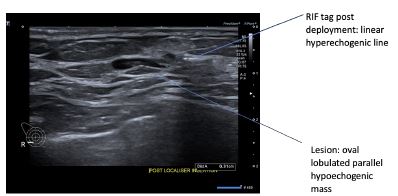
Figure 4: Axial Ultrasound image post deployment of the RIF tag, with the lesion and RIF tag in situ. The distance measured is the distance between the lesion and the RIF tag.

Figure 5: Labelled ultrasound image depicting RIF tag and lesion.
SAVI SCOUT technology involves the insertion of an electromagnetic wave reflector into the breast under image guidance [5]. A handheld probe generates infrared impulses which activate the reflector and this causes an electromagnetic wave signal to be reflected back, guiding the surgeon to the lesion that needs to be removed. The reflectors used are not radioactive, and provide an accurate detection range up to 6 cm, again posing a problem in bigger, more dense breast tissue [6].SAVI SCOUT offers a large advantage in that it causes significantly less artefact on MRI than that of RFID tags and Magseeds, giving it more viability in terms of long-term surveillance and monitoring scans [6].
The Magseed technique [7] involves deploying a 5mm paramagnetic steel seed under image guidance into the breast. The handheld probe magnetizes the seed and creates a magnetic field, allowing for real time localization of the seed and lesion. The seed can be inserted into the breast at any time, and has been shown to aid localization for lesions reliably at 4 cm depth (with some further lesions being detected up to 12 cm depth). A big drawback to the Magseed technique is that it causes significant artefact on MRI, making its use limited in assessing a patient’s response to neoadjuvant chemotherapy. A systematic review conducted by Gera et al [7] analyzed 1559 magseeds cases in 16 studies and showed successful placement rate of 94.42% and a successful localization rate of 99.86%. Four studies were analyzed in a separate pooled analysis and showed no statistically significant difference between re-excision rates using Magseeds and WGL.
Figure 6 below demonstrates a Magseed introducer and device.

Figure 6: Magseed introducer + device [8].
In this paper, we compared the use of wires to Radiofrequency (RFID) tags in the localization of non-palpable breast lesions. As shown in our results Table 1, the wire cases had to have wire inserted on the same day as surgery, whereas the RFID tags were inserted anywhere from 6 to 55 days before surgery, allowing for greater preoperative flexibility and scheduling. A large part of patient anxiety is avoided by scheduling these procedures separately rather than adding to the stress on the day of surgery. The RFID tags provide an alternative localization technique compared to the wires, demonstrating accurate localization of lesions. Finally, the average specimen weight for wire cases was 51 g, compared to 57 g for tag cases, showing roughly similar specimen sizes.
A systematic review conducted by Tayeh et al [9] examines 1151 patients and the use of 1344 tags, and found re-excision rate to be 13.9% amongst these cases. Two studies compared RFID with WGL (128 vs. 282 patients respectively), and for both of these techniques the re-excision rate was 15.6% (20/128 vs. 44/282 respectively, p value is 0.995).
We have found in our study that radiofrequency localization technology offers an effective alternative to localization methods for non-palpable breast lesions when compared to wire guided localization. RFID tags offer increased accuracy of excision, with the probe guiding exact distance to the lesion, but it causes problems with MRI imaging and patients with pacemakers. WGL is more well known amongst surgeons, requiring less equipment and training, but we would recommend the increased use and training into alternative wire free localization methods to overcome this.
Another important aspect to consider when comparing these alternative localization methods is the relative cost of each technology. NICE guidance [10] published in 2020 states that each Magseed unit costs £250 per single-use Magseed (with an additional cost of £25000 per reusable Sentimag probe), compared to the £35-£50 cost for wire guided technology. The main barrier to the use of Magseed has thus far been quoted as the cost of each seed and the probe, however, a service evaluation [10] done has shown a cost saving of £34,457 with Magseed compared to traditional wire guided localization, with improved efficiency of clinics, and reduced number of re-excision cases. With regards to the cost of RFID, there is general anecdotal evidence that the cost of RFID technology is more expensive than wire guided localization, but further studies are needed to evaluate the cost-effectiveness of these alternative technologies as this will be of paramount importance when considering the implementation of these technologies into the NHS system.
Finally we have reviewed a large meta-analysis study that evaluated Non Wired Non-Ionising (NWNI) preoperative localizations techniques for non-palpable breast cancers [11]. This study found that the positive margin rate was lower for NWNI techniques and it offered a lower re-excision rate when compared to WGL but these results were not statistically significant. For future research, we need larger multicenter studies with bigger patient numbers to draw more conclusions from these data sets. There is also a lack of randomized studies reporting on these outcomes, which limits the conclusions that can be drawn about the efficacy of these methods.
Conclusion
Our study demonstrates that radiofrequency localizations technology is an effective and comparable alternative to wire-guided localizations, with the added advantage of decoupling surgery and radiology scheduling.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71: 209-249. 10.3322/caac.21660
- Frank HA, Hall FM, Steer ML. Preoperative localization of nonpalpable breast lesions demonstrated by mammography. N Engl J Med. 1976; 295: 259-260. 10.1056/NEJM197607292950506
- Kapoor MM, Patel MM, Scoggins ME. The Wire and Beyond: Recent Advances in Breast Imaging Preoperative Needle Localization. Radiographics. 2019; 39(7): 1886-1906. 10.1148/rg.2019190041
- Wazir U, Tayeh S, Perry N, Michell M, Malhotra A, et al. Wireless Breast Localization Using Radio-frequency Identification Tags: The First Reported European Experience in Breast Cancer. In Vivo. 2020; 34(1): 233-238. doi:10.21873/invivo.11765
- Kasem I, Mokbel K. Savi Scout(R) Radar Localisation of Non-palpable Breast Lesions: Systematic Review and Pooled Analysis of 842 Cases. Anticancer Res. 2020; 40: 3633-3643. 10.21873/anticanres.14352
- Wazir U, Kasem I, Michell MJ, et al. Reflector-Guided Localisation of Non-Palpable Breast Lesions: A Prospective Evaluation of the SAVI SCOUT® System. Cancers (Basel). 2021; 13(10): 2409. doi:10.3390/cancers13102409
- Gera R, Tayeh S, Al-Reefy S, Mokbel K. Evolving Role of Magseed in Wireless Localization of Breast Lesions: Systematic Review and Pooled Analysis of 1,559 Procedures. Anticancer Res. 2020; 40:1809-1815. 10.21873/anticanres.14135
- Med Gadget. The Magseed Injectable Marker: Interview with Eric Mayes, CEO of Endomag. 2018. Accessed: November 15, 2023, with permission: https://www.medgadget.com/2018/03/magseed-injectable-marker-interview-eric-mayes-ceo-endo mag.html
- Tayeh S, Wazir U, Mokbel K. The Evolving Role of Radiofrequency Guided Localization in Breast Surgery: A Systematic Review. Cancers (Basel). 2021; 13. 10.3390/cancers13194996
- Magseed for locating impalpable breast cancer lesions. Accessed: April 26, 2024: https://www.nice.org.uk/advice/mib236/resources/magseed-for-locating-impalpable-breast-cancer-lesions-pdf-2285965575839941#:~:text=Magseed%20(Endomag)%20is%20a%20marker,of%20 surgical%20grade%20stainless%20steel.
- Garzotto F, Comoretto RI, Michieletto S, et al. Preoperative non-palpable breast lesion localization, innovative techniques and clinical outcomes in surgical practice: A systematic review and meta-analysis. Breast. 2021; 58: 93-105. doi:10.1016/j.breast.2021.04.007