Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Nobuhiko Aoki*
*Corresponding Author: Nobuhiko Aoki
Department of Neurosurgery, Bethlehem Garden Hospital 3-14-72 Umesono, Kiyose, Tokyo 204-0024, Japan.
Tel: +81-42-401-2525 & +81-42-495-2878;
Email: aoki.bb@jiseikai.jp
Article Info
Received: Oct 25, 2024
Accepted: Nov 13, 2024
Published: Nov 20, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Aoki N (2024).
Abstract...
Background: An Acute Subdural Hematoma (ASDH) in an infant without external signs of head trauma is diagnosed as Shaken Baby Syndrome (SBS) in the United States or as an Infantile Acute Subdural Hematoma (IASDH) due to minor head trauma in Japan. The present case report analyzes the pre- and post-operative neuroimaging findings of fulminant-type IASDH and demonstrates that this condition can resolve fully with prompt surgery.
Case description: A 9-month-old, male infant fell at home while trying to stand up by holding on to a sofa. He struck his occipital region on a mat and began crying. Soon thereafter he displayed signs of altered consciousness status and seizure-like activity. He was taken to an emergency room by ambulance where head Computed Tomography (CT) revealed a left-sided, holohemispheric, subdural collection with a remarkable midline shift.
The patient’s conscious status deteriorated rapidly, requiring an emergency craniotomy. Intraoperatively, bloody fluid gushed out, and a partially clotted hematoma was removed. The origin of the hemorrhage was unable to be determined. His postoperative course was favorable without any neurological deficits. Fundoscopic examination revealed a left-sided retinal hemorrhage.
Postoperative CT on day 1 visualized a thin line indicative of a Subdural Hematoma (SDH) with resolution of the mass effect. Magnetic Resolution Imaging (MRI) on day 16 revealed a thin, tapering SDH. CT on day 34 found a tiny, film-like hemorrhage.
The patient was followed up on an outpatient basis for more than two years but did not present any neurological abnormalities.
Conclusion: The present case is invaluable because it demonstrates that the outcome of emergency surgery and the ensuing recovery of fulminant-type IASDH can be favorable in the absence of a cerebral parenchymal injury. Particularly relevant here is the thin, film-like image observed after evacuation of the ASDH, which likely indicated the localization of the hemorrhage in the Dural Border Cell Layer (DBCL). Based on the serial neuroimaging analysis, the fulminant-type IASDH was considered secondary to the spread of the hemorrhage in the BDCL into the subdural compartment.
Keywords: Infantile acute subdural hematoma; Shaken baby syndrome; Abusive head trauma; Benign enlargement of subarachnoid space; Large sylvian fissure; Holohemispheric hemorrhage; Dural border cell layer; Cerebral parenchymal injury.
Citation: Aoki N. Fulminant-Type Infantile Acute Subdural Hematoma: Pre- and Post-operative Neuroimaging Analysis. J Clin Med Surgery. 2024; 4(2): 1173.
Introduction
Infantile Acute Subdural Hematomas (IASDH) have been reported in Japan since the 1960’s [1]. However, because most reports were published in Japanese-language journals, coupled with the frequent criticism that the diagnosis was being used to conceal cases of child abuse, the concept of IASDH was not widely accepted in the English-speaking world [2,3].
Fulminant-type IASDH is the most severe form of IASDH and differs from Shaken Baby Syndrome (SBS) in that it does not involve a cerebral parenchymal injury [1,4,5]. As far as was able to be ascertained, no previous studies have discussed the neuroimaging characteristics of fulminant-type IASDH. The present study therefore aimed to clarify the neuroimaging features and treatment for fulminant-type IASDH.
Case presentation
A 9-month-old, male infant with no remarkable medical history fell and struck his occipital region at home while trying to stand up by holding on to a sofa. He began crying and soon thereafter vomited and displayed signs of altered consciousness status accompanied by seizure-like activity. He was taken to an emergency room by ambulance. On arrival, head Computed Tomography (CT) revealed a left-sided, mixed-density subdural hematoma with a remarkable midline shift to the right. In addition, an enlarged Sylvian Fissure (LSF) was noted on the right side (Figure 1). His conscious status deteriorated rapidly, requiring emergency surgery. Intraoperatively, bloody fluid gushed out, and a partially clotted hematoma was removed.
The origin of the hemorrhage was unable to be identified within the surgical field. His postoperative course was uneventful, and he achieved recovery without any neurological deficits. Fundoscopic examination revealed a left-sided, retinal hemorrhage.
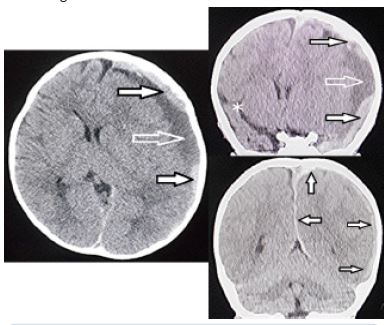
Figure 1: Computed tomography 3 hours after presentation.
Upper: Axial view, Middle & Lower: Coronal view.
Upper & Middle: High density (black arrows) and low density (white arrow) components of the left-sided subdural hematoma (SDH). Note the remarkable midline shift to the right side and the large sylvian fissure on the right side (asterisk).
Lower: SDH covering the entire cerebral hemisphere (i.e, holohemispheric hemorrhage) on the right side (pink arrows)
Upper: Axial view, Middle & Lower: Coronal view.
Upper & Middle: High density (black arrows) and low density (white arrow) components of the left-sided subdural hematoma (SDH). Note the remarkable midline shift to the right side and the large sylvian fissure on the right side (asterisk).
Lower: SDH covering the entire cerebral hemisphere (i.e, holohemispheric hemorrhage) on the right side (pink arrows)
CT on postoperative day 1 visualized a thin line indicative of a high-density lesion as well as resolution of the mass effect (Figure 2). Magnetic Resonance Imaging (MRI) on day 16 revealed a thin, high-intensity SDH covering the entire left cerebral hemisphere. No parenchymal abnormality indicating a primary brain injury was found (Figure 3). CT on day 34 found a tiny, film-like hemorrhage at the inner table of the frontal bone (Figure 4). The patient was followed up on an outpatient basis for more than two years but presented no neurological abnormalities.
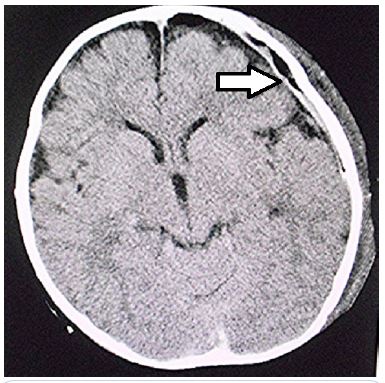
Figure 2: Computed tomography on postoperative day 1.
Resolution of the midline shift and the thin, linear, high-density lesion on the left side can be seen (arrow).
Resolution of the midline shift and the thin, linear, high-density lesion on the left side can be seen (arrow).
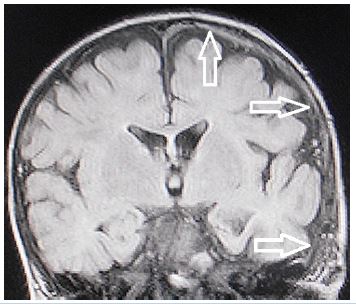
Figure 3: Magnetic resonance imaging (fluid-attenuated inversion recovery, coronal view) on postoperative day 27.
The thin, high-intensity subdural hematoma can be seen covering the entire cerebral hemisphere on the left side (arrows). No parenchymal abnormality indicating primary brain injury was observed.
The thin, high-intensity subdural hematoma can be seen covering the entire cerebral hemisphere on the left side (arrows). No parenchymal abnormality indicating primary brain injury was observed.
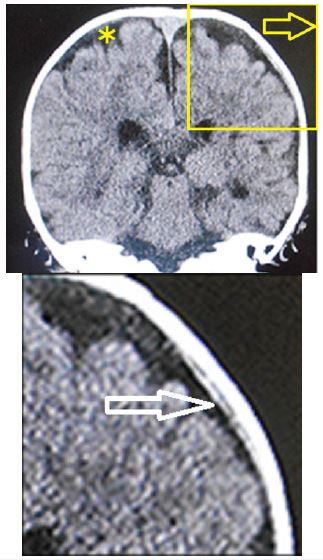
Figure 4: Coronal view on computed tomography on postoperative day 3.
Left: Full-sized view.
Right: Enlargement of the area in the box on the full-sized view.
The thin, film-like, high-density lesion corresponding to the hemorrhage (arrow) can be seen in the dural border cell layer. Note the benign enlargement of the subarachnoid space on the full-sized view (asterisk).
Left: Full-sized view.
Right: Enlargement of the area in the box on the full-sized view.
The thin, film-like, high-density lesion corresponding to the hemorrhage (arrow) can be seen in the dural border cell layer. Note the benign enlargement of the subarachnoid space on the full-sized view (asterisk).
Table 1: Comparison of Infantile Acute Subdural Hematoma (IASDH) and Shaken Baby Syndrome (SBS) / Abusive Head Trauma (AHT).
| IASDH | SBS/AHT | |
|---|---|---|
| Applied force | Minor headtrauma | Abuse (highenergy impact) |
| Main etiology | Disruption of the bridging vein | Cerebral contusional tears |
| Primary brain injury | None | Common |
| Age distribution | Peak at 6 - 10 months | Widely distributed (including less than3 months) |
| Sex | Marked preponderance in males | No preponderance |
| Recurrence | Rare | Not rare |
| Prognosis | Depends on hematoma volume(mostly benign clinical courses) | Poor |
| Retinal hemorrhage | Frequent | Common |
Note: (Cited from Ref. 1 with permission of the Society of Japanese Neurosurgery)
Table 2: Clinical grade of infantile acute subdural hematoma on the arrival of patients at the emergency department; proposed in 1984 (Ref. 4).
| Grade | Type | Clinical features |
|---|---|---|
| I | Mild | Conscious, no motor disturbance. Vomiting and/orirritability present |
| II | Intermediate | Drowsiness, minimalor mild hemiparesis |
| III | Fulminant | Stupor to coma, moderate to severe hemiparesis.Signs of cerebral herniation present |
Discussion
Based on the biophysiological characteristics of infants, IASDH was originally defined in 1984 as an acute, infantile subdural hematoma apparently caused by minor head trauma without loss of consciousness and not associated with a primary brain injury [4]. Most cases of IASDH are also associated with retinal hemorrhage [4].
IASDH is clinically graded as mild (grade I), intermediate (grade II) or fulminant (grade III) in accordance with the findings of a previous study (Table 1) [4]. The pathological features of IASDH, including the fulminant type, as indicated by imaging studies and surgical findings, account for its mostly benign clinical course following conservative management or prompt surgical intervention [5-7]. It is important to emphasize that a favorable outcome depends greatly on the absence of a primary cerebral parenchymal injury. As far as could be ascertained, however, no English-language studies to date have discussed primary cerebral parenchymal injury as a feature differentiating IASDH from SBS (Table 2).
The Dural Border Cell Layer (DBCL), a distinct, soft-tissue layer at the dural-arachnoid interface, is composed of a loose conglomeration of cells having enlarged, extracellular spaces and no extracellular collagen [8]. ASDH occurring in this environment results from the disruption of the DBCL by pooled blood. Furthermore, in the superficial compartment of the DBCL, there is a well-developed dural venous plexus which fills the venous sinuses. Because the DBCL is easily disrupted, a hemorrhage originating in the inner dural plexus may be chiefly responsible for the non-traumatic symptoms of this condition [9]. Particularly relevant here is the thin, film-like image on CT which is observable after evacuation of the ASDH and which may indicate the localization of the hemorrhage in the DBCL [10,11].
Based on the serial neuroimaging analysis in the present patient, the fulminant- type IASDH was considered secondary to the spread of the hemorrhage from the DBCL into the subdural compartment; the tiny, film-like hemorrhage at the inner table of the frontal bone on CT on postoperative day 34 coincided to be trapped in the DBCL [12] (Figure 4).
Conclusions
The present case is invaluable because it demonstrates that emergency surgery can produce a favorable outcome in fulminant-type IASDH in the absence of a cerebral parenchymal injury, the fundamental feature distinguishing IASDH from SBS. Particularly relevant here is the thin, film-like appearance observed after evacuation of the ASDH, which likely indicated the localization of the hemorrhage in the DBCL. Based on serial neuroimaging analysis results, fulminant-type IASDH was considered secondary to the spread of the hemorrhage from the DBCL into the subdural compartment.
Declarations
Author contribution: Nobuhiko Aoki (corresponding author with no coauthors) conceived the study, conducted a search of the literature, and drafted the original manuscript. The author has reviewed the manuscript draft, revised it critically for intellectual content, and approved the final version for submission.
Availability of data and materials: This article does not include any data or material that can be provided.
Declarations, ethics approval, and consent to participate: This article was approved by the ethics committee of Bethlehem Garden Hospital and Tokyo Metropolitan Tama Medical Center. No funding was obtained for this study. The parents/legal guardians of the patient provided their consent to publish the details of this case.
Consent to publish: The author consents to the publication of all identifiable details, which may include photographs, case history, and other details.
Conflicts of interest: None.
References
- Aoki N. Infantile acute subdural hematoma: Caused by abuse or mild head trauma? Nervous System in Children. 2011; 36: 326-330.
- Rekate HL. Subdural hematomas in infants. (Letter) J Neurosurg. 1985; 61: 316-317.
- Wittschieber B, Karger D, Pfeifer H. Understanding Subdural Collections in Pediatric Abusive Head Trauma. AJNR AmJ Neuroradiol. 2019; 40: 388-395.
- Aoki N, Masuzawa H. Infantile acute subdural hematoma. Clinical analysis of 26 cases. J Neurosurg. 1984; 61: 273-280.
- Aoki N. “Infantile” acute subdural hematoma: A clinical entity different from abusive head trauma. J Pediatr Neurol Neurosci. 2020; 4: 151-53.
- Aoki N. Clinical and neuroimaging characteristics in mild-type infantile acute subdural hematoma. Report of four cases. Childs Nerv Syst. 2023; 40(1): 189-195.
- Aoki N. Infantile acute subdural hematoma. Clinical and neuroimaging analysis of 15 cases focusing on intracranial structural vulnerabilities. Journal of Surgery. 2024. DOI: 10.2901112575-97
- Nabeshima S, Reese TS, Landis DM, et al. Junctions in the meninges and marginal glia. J Comp Neurol. 1975; 164: 127-169.
- Mack J, Squier W, Eastman JT. Anatomy and development of the meninges: Implications for subdural collections and CSF circulation. Pediatr Radiol. 2009; 391: 200-210.
- Aoki N. Holohemispheric subdural hematoma: Infantile acute subdural hematoma localized in the dural border cell layer. Ann Case Report. 2024; 9: 1959. DOI:10.29011/2574-7754.1019598
- Aoki N. Mild-type infantile acute subdural hematoma presenting with a holohemispheric subdural hematoma. Ame J Surg Clin Case Rep. 2024; 8(2): 1-5.
- Aoki N. Holohemispheric Hemorhhage in Infantile Acute Subdural Hematoma: Serial Neuroimaging Analysis, J. Neuroscience and Neurological Surgery. 2024; 14(8). DOI:10.31579/2578-8868/341