Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Eugenia Lin1*; Andrea Leyton-Mange2; John Andrawis3; Meredith G Moore4; Kevin J Bozic5; Edison Thomaz6; Prakash Jayakumar7
*Corresponding Author: Eugenia Lin
Department of Orthopedic Surgery, Mayo Clinic Arizona Phoenix, Arizona, USA.
Email: lin.eugenia@mayo.edu
Article Info
Received: Oct 08, 2024
Accepted: Nov 01, 2024
Published: Nov 08, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Lin E (2024).
Abstract...
Objectives: Studies examining the relationship between physical activity data generated by wearable sensors from patients undergoing orthopaedic surgical procedures and capability (measured using patient reported outcome measurements or PROMs) are lacking. The primary objective was to assess the correlation between preoperative activity data from wearables and baseline capability (KOOS JR and HOOS JR) in patients with osteoarthritis undergoing Total Joint Arthroplasty (TJA) for knees or hips. Secondarily, we assess the correlation between pre-operative wearable activity data and baseline depression, general physical health and mental health, and six-week postoperative capability.
Methods: In this pilot study we prospectively recruited forty-eight patients at an academic medical center undergoing TJA and provided them with wearable sensors (Fitbit Charge 2 or Fitbit Alta) at least six weeks prior to their procedure. We tracked wearable sensor generated daily step counts, durations of activity, and sedentary behavior. We collected measures of capability (KOOS JR, HOOS JR), general physical and mental health (PROMIS Global-10), and symptoms of depression (Patient Health Questionnaire-2) preoperatively. Capability was also assessed postoperatively at six weeks.
Results: Pre-operative daily step count, activity minutes, and sedentary minutes captured using wearables were not associated with baseline capability. A greater number of pre-operative daily steps were associated with fewer symptoms of depression (ρ=-0.49, P=0.03) and greater preoperative general physical health (r(18)=0.49, P=.03). Greater preoperative wearable-derived daily activity minutes were also negatively associated with symptoms of depression (ρ=-0.49, P=0.03). No associations were found between baseline wearable activity and six-week level of capability.
Conclusion: The association between wearable-sensor generated markers of activity with pre-operative psychological distress and pre-operative general physical health signal opportunities to use this technology to passively assess health status and reduce the survey burden on patients undergoing joint replacement surgery. Further work is required to validate wearable sensor technology for clinical decision support and shared decision making.
Keywords: Knee; Hip; Osteoarthritis; Arthroplasty; Wearables.
Citation: Lin E, Leyton-Mange A, Andrawis J, Moore MG, Bozic KJ, et al. The Relationship Between Activity Captured Using Wearable Sensors and Capability in Patients Undergoing Total Joint Replacement. J Clin Med Surgery. 2024; 4(2): 1171.
Introduction
Osteoarthritis (OA) of the hip and knee is a leading cause of disability, estimated to impact around 240 million people worldwide including more than 32 million adults in the U.S [1]. Those with severe OA can be managed with Total Knee Arthroplasty (TKA) and Total Hip Arthroplasty (THA), procedures that are shown to consistently alleviate pain, restore mobility, and increase quality of life [2,3]. Patient-Reported Outcome Measures (PROMs) are validated surveys designed to actively capture a patient’s perception of capability and comfort related to a health condition. These tools have been used extensively in the evaluation of outcomes following TKA and THA [4-6]. The digitization of PROMs collection using online platforms and devices such as tablets and smartphones has made it easier to collect and integrate the data from these tools into electronic medical records of patients. However, active capture of such patient generated health data can pose a survey burden on patients and administrative challenges to health systems [5,7]. Greater access to consumer-grade wearable sensors, such as smartwatches and activity trackers, has made it feasible to use these tools to collect real-time activity data in post-surgical patients [8]. Though recent studies have assessed the correlation between PROMs with activity-related metrics from wearable sensors, knowledge gaps remain around the feasibility of wearables to assess an individual’s health status in different clinical settings, and the relationship between metrics generated by these tools with other health domains, such as psychosocial factors. Thus, we were interested in assessing the correlation between wearable-derived activity data from commercially available Fitbit devices and PROMs capturing capability as well as general physical and mental health in patients with hip or knee OA undergoing joint replacement surgery. The primary objective of this study was to assess the association between preoperative (baseline) wearable activity data (step count, activity minutes, and sedentary minutes) with baseline capability (HOOS JR and KOOS JR). Secondarily we assess the relationship between baseline wearable- activity data with baseline symptoms of depression, general physical health, and general mental health. Finally, we assess the relationship between baseline wearable activity data and six-week postoperative capability.
Methods
Study design and sampling
We performed a prospective study involving the recruitment of a consecutive series of adult patients at an academic orthopaedic clinic. We included new adult patients aged 18 years or older presenting with OA of the hip or knee undergoing THA or TKA respectively. Patients were required to have a smartphone device to allow installation of the FitBit mobile application to pair with, store, and enable efficient upload of data generated by the wearable component (a FitBit personal digital device worn on the wrist). We acquired study approval from our local Institutional Review Board and enrolled 48 patients after acquiring informed consent.
We extracted demographic data, preoperative and six-week postoperative Hip Disability and Osteoarthritis Outcome Score – Joint Replacement (HOOS JR) or Knee Injury and Osteoarthritis Outcome Score- Joint Replacement (KOOS JR) scores, and the date of surgery from the electronic health records (Athenahealth, Watertown, MA, USA). We provided participants in the study with one of two commercially available, wrist-based activity trackers (Fitbit Charge 2 or the Fitbit Alta, Fitbit, San Francisco, CA, USA) at enrollment. Research assistants educated study participants on wearable use and maintenance, such as charging the wearable, and requested patients to wear the device daily from the initial (or baseline) clinical appointment until their six-week postoperative visit. Deidentified data captured by the activity tracking device was transmitted wirelessly to the Fitbit companion mobile application and subsequently uploaded to the Fitbit servers using a secure and encrypted connection. Researchers installed the mobile application on participants’ phones and paired each device with this application at the time of study enrollment. Research team members accessed participants’ data through a third-party interface to the Fitbit servers; this interface was provided by Fitabase (Fitabase, San Diego, CA, USA).
TJRs were performed by one of three surgeons and all patients underwent standard clinical preoperative and postoperative protocols as designated by surgeons and current standard-of-care.
Measures
Fitbit (Charge2 and Alta): Fitbit Charge 2 and Fitbit Alta are consumer-grade, wireless-enabled activity trackers released by Fitbit in 2016. The activity trackers are worn on the wrist and designed for daily general use with wearable sensors that collect activity metrics including hourly and daily step counts, distance covered, calories burned, and number of minutes designated by Fitbit’s software algorithm.
Patient-Reported Outcome Measures (PROMs): We collected PROMs data for all subjects from the electronic medical record. At the preoperative surgical consultation visit, the Patient Health Questionnaire 2 (PHQ-2), PROMIS Global Health-10, and either the HOOS JR or KOOS JR for patients undergoing THA or TKA respectively were collected. PHQ-2 is a widely used, validated screening tool for symptoms of depression. PROMIS Global-10 is a general health survey reflecting quality of life, providing two separate interval scores for general physical health and general mental health with ranges from 16.2-67.7 and 21.2-67.6, respectively. Higher scores reflect greater quality of life in either the mental or physical domain. HOOS JR and KOOS JR are specific to TJA and specifically measure hip and knee specific function using interval scores encompassing pain, physical function, and stiffness with ranges from zero-100. A score of 100 reflects no limitations while 0 reflects maximum limitations. The HOOS JR and KOOS JR were also collected at the six-week postoperative visit.
Data collection
`Data was securely collected and managed using HIPAA-compliant, research database software, REDCap™ (Research Electronic Data Capture) [9,10].
Inclusion eligibility for data analysis
First, we determined the eligibility of inclusion of Fitbit data points per subject by examining the calories burned. We utilized the hourly calorie metric to determine whether the device was worn on a given day. If a caloric metric above baseline calorie was noted for at least 50% (or ≥8 hours) of waking hours (16 hours), this was considered as an included day of wear. Subjects included based on these criteria were further examined to ensure sufficient preoperative data and excluded if there was not at least three days of preoperative wearable data. Excluding the days for which no data was transmitted and date of surgery, the daily average of steps, minutes, distance, and activity levels were computed in the Fitbit-designed categories of very active, moderately active, light active, and sedentary for the respective daily averages.
Statistical analysis
We analyzed all data using STATA 16.1 (Statacorp, College Station, TX, USA). We performed descriptive statistics to summarize patient characteristics and Spearman’s correlation (ρ) and Pearson’s product-moment correlation (R) to assess the relationship between preoperative wearable-data and baseline capability as well as further analyses to assess the relationships between preoperative wearable activity data and baseline measures of symptoms of depression, general physical and mental health, and six-week postoperative capability.
Results
We recruited a total of 48 patients from March 2018 through March 2019. A total of 28 patients had incomplete data insufficient for analysis, withdrew from the study, or did not undergo surgery (Figure 1). The final study cohort for analysis of this pilot study included 20 patients. The mean age of this cohort was 63 years and primarily women (65%) (Table 1).
No significant associations were found between baseline wearable activity data, including daily steps, activity minutes, or sedentary time, with baseline capability.
Greater baseline step count was significantly associated with lower levels of pre-operative depression (ρ=-0.49, P=0.03) and greater levels of aggregated pre-operative physical activity minutes were associated with lower levels of preoperative psychological distress (ρ=-0.49, P=0.03) (Table 1).
Greater baseline daily step count was associated with greater preoperative general physical health (r(18)=0.49, P=.03).
Finally, there were no associations found between preoperative wearable activity data and six-week postoperative hip or knee capability (Table 2).
Table 1: Patient demographics for included cohort of patients.
| Variable | Value |
|---|---|
| N | 20 |
| Age, years | 62.9±8.4 |
| Gender | |
| Men | 7(35%) |
| Women | 13(65%) |
| Race/ethnicity | |
| White | 16(80%) |
| Hispanic | 1(5%) |
| Asian | 1(5%) |
| Black or AfricanAmerican | 1(5%) |
| Other | 1(5%) |
| Index Surgery | |
| Right THA | 4(20%) |
| Left THA | 3(15%) |
| Bilateral THA | 2(10%) |
| Right TKA | 3(15%) |
| Left TKA | 6(30%) |
| Bilateral TKA | 2(10%) |
| Preoperative PROMISGlobal 10 | |
| Physical Health | 43.1±9.4 |
| Mental Health | 53.0±6.8 |
| Preoperative PHQ-2 | |
| Positive | 2(10%) |
| Negative | 18(90%) |
| Preoperative HOOS JR | 51.6±16.4 |
| Preoperative KOOS JR | 53.0±12.6 |
| 6-week postoperative HOOS JR | 85.9±16.9 |
| 6-week postoperative KOOSJR | 61.8±8.7 |
| Preoperative sensordata | |
| Daily steps | 6304.6±3121.8 |
| Daily activity minutes | 232.7±89.3 |
| Daily sedentary time | 917.8±203.8 |
| Days with steps | 73.8±69.8 |
| Discrete variables as number (percentage); continuous variables as mean ± standard deviation or median (interquartile range). | |
Table 2: Correlation between fitbit data measures and patient-reported outcome measures, preoperatively and 6-weeks postoperatively.
| Preoperative wearable data | ||||||
|---|---|---|---|---|---|---|
| Step Count | Activity Minutes | Sedentary Minutes | ||||
| Categorical variables | Spearman correlation (ρ) | P-value | Spearman correlation (ρ) | P-value | Spearman correlation (ρ) | P-value |
| PHQ-2 | -0.49 | 0.03* | -0.49 | 0.03* | 0.26 | 0.26 |
| Continuous variables | Pearson correlation (r) | P-value | Pearson correlation (r) | P-value | Pearson correlation (r) | P-value |
| Preoperative HOOSJR | 0.54 | 0.14 | 0.41 | 0.27 | -0.31 | 0.42 |
| Preoperative KOOSJR | 0.12 | 0.71 | -0.29 | 0.38 | 0.07 | 0.84 |
| Preoperative PROMISGlobal 10 Physical | 0.49 | 0.03* | 0.29 | 0.22 | -0.11 | 0.63 |
| Preoperative PROMISGlobal 10 Mental | 0.18 | 0.46 | 0.16 | 0.49 | -0.06 | 0.79 |
| 6-week HOOS JR | 0.49 | 0.18 | 0.51 | 0.17 | -0.01 | 0.97 |
| 6-week KOOS JR | 0.45 | 0.16 | 0.19 | 0.58 | 0.003 | 0.99 |
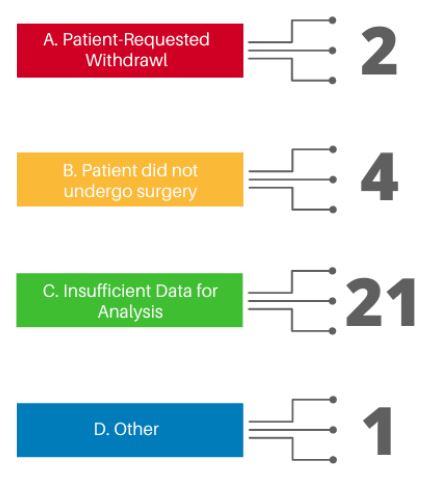
Figure 1: Patient exclusion from final cohort for data analysis.
This figure shows the reasons for patient exclusion from the final cohort of subjects used for data analysis. Numbers represent the number of patients in each category.
Discussion
Findings
Increased adoption of wearable technologies to track and monitor activity levels provides an opportunity for clinicians to track health status passively without burdening patients with surveys while also enabling clinicians to understand a patient’s behavior outside the clinic setting and within their usual environment. In this pilot study, we examined the correlation between activity levels collected using wearable sensors and PROMs of capability.
Firstly, we observed that there were no associations between preoperative wearable activity metrics and capability in patients with hip or knee OA undergoing TJA. This could be a result of the relatively small sample size in this pilot study, a short duration of follow-up, and a level of imprecision from analyzing aggregated data using proprietary algorithms from consumer-grade wearables. Studies to date validating consumer-grade wearables following TJA also show mixed results including inaccuracies within the capture of activity metrics such as distance [11,12] and step counts [13]. Analysis using the raw wearable-generated data (such as that generated by research grade wearables) with specific statistical techniques to reduce noise and spurious elements in the data, rather than aggregate scores generated using proprietary algorithms may yield alternative findings. Notably, machine learning has also been applied to patient generated health data from wearables to better predict outcomes and risk stratify patients to align them with treatment options [14,15]. Prior studies using PROMs showed that preoperative PROM scores were able to predict pain and function after total joint replacement but only at longer durations of follow-up [16-19]. Studies also suggest that functional status for patients during the six-week postoperative period after TJA declines before improving [20,21]. Thus future work using wearable activity tracking should account for this recovery trajectory and assess change and associations at different time points over longer durations i.e., beyond early rehabilitation toward return to usual activity and maintenance.
We also found that psychological distress correlates with lower baseline activity levels and step counts, and physical health related quality of life correlates with higher daily step counts. These associations demonstrate the potential utility of wearable activity trackers to passively and continuously capture some important domains of physical and emotional health and wellbeing in their usual environment. This approach confers an advantage over PROMs which often increase the responder burden and ultimately serve as static snapshots of health status at discrete points in time.
Strengths and limitations
In this study, we examined different types of wearable activity data, such as activity level and sedentary level, beyond traditional accelerometer-based step-counts often used in prior literature. A range of different metrics captured continuously yields a more granular and voluminous set of data points for analysis. Using not only condition-specific PROMs, but also broader psychosocial and general health measures in conjunction with this wearable activity data enables a more holistic evaluation of the patient’s health status.
There were several limitations to this study. Firstly, we experienced a substantial drop-off from patient enrollment to inclusion of the subject data in analysis, resulting in a small sample size. Future studies should involve larger cohorts and address potential issues related to adherence and the feasibility of capturing wearable-generated data over longer durations of time. Qualitative studies assessing patient experiences could yield some rich insights into the barriers and facilitators of this mode of capturing health status. Second, selection bias may exist in this study for more technologically minded patients in adhering to the study protocol and complying with the use of wearables over those that may be less familiar or comfortable with the technology. A better understanding of the digital preferences and digital literacy of diverse populations with this mode of data capture might better inform future study designs using this technology. Third, this pilot study also included a limited number of patients recruited from an academic medical center and thus may not be generalizable to other populations. Notably, the final cohort of our patients does not reflect the diversity of our usual clinic population. The sample of patients were predominantly white where our broader clinical population usually includes a substantial Hispanic population. Fourth, we had difficulty accessing raw sensor data for analysis, as the data was stored and transmitted through Fitbit’s proprietary applications.
Thus, we were unable to analyze metrics outside of the generated algorithms. This, however, is a general limitation of any research involving commercial-grade personal digital devices incorporating wearable sensors. Finally, we did not collect postoperative psychosocial or general health PROMs, and thus we could not assess change in mental health and quality of life between preoperative and postoperative time points [2,22]. Finally, patient medical history and conditions, such as the reason for total joint replacement or BMI, was not examined. We were thus not able to account for these additional clinical variables.
Conclusion
Patient-generated health data collected by wearables afford clinicians an opportunity to better understand and predict patient health outcomes in their usual environment while reducing the burden of surveys on the patient. Psychosocial factors are a dominant driver of patient comfort and capability across a range of health conditions. While our study did not find associations between preoperative wearable activity and baseline capability, we did demonstrate that baseline measures of symptoms of depression were negatively correlated with preoperative daily step counts and activity levels. We also found higher general physical function was positively correlated with preoperative daily step counts. Wearable technology continues to evolve with increased sophistication of sensors and greater opportunities to access to raw data through open-source algorithms. Future work should evaluate the barriers and facilitators of using these tools to capture health status among diverse populations as well as validate the data generated from these devices at scale with other markers of activity and behavior.
Declarations
Conflict of interest: No declaration of conflict of interest in this manuscript.
Funding: All authors certify that there are no funding or commercial associations that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. No forms of financial support including grants were received by the authors for the support of this study in preparation, research, authorship, and publication of this manuscript.
Ethical approval for study: Ethical approval by the University of Texas at Austin Institutional Review Board was obtained for this study (Protocol Number: 2017-11-0008).
Informed consent: There are no information in the submitted manuscript that can be used to identify patients.
Acknowledgement: We would like to acknowledge Lauren Uhler and Tyler Goldberg for their work in coordination for this project.
References
- Katz JN, Arant KR, Loeser RF. Diagnosis and Treatment of Hip and Knee Osteoarthritis. JAMA. 2021; 325(6): 568. doi: https: //doi.org/10.1001/jama.2020.22171
- Ethgen O, Bruyère O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty: a qualitative and systematic review of the literature. JBJS. 2004; 86(5): 963-74.
- Jones CA, Voaklander DC, Johnston DW, Suarez-Almazor ME. Health related quality of life outcomes after total hip and knee arthroplasties in a community based population. The Journal of rheumatology. 2000; 27(7): 1745-52.
- Greenhalgh J, Dalkin S, Gooding K, Gibbons E, Wright J, et al. Functionality and feedback: A realist synthesis of the collation, interpretation and utilization of patient-reported outcome measures data to improve patient care. Health Services and Delivery Research. 2017; 5(2): 1-280.
- Jensen RE, Rothrock NE, De Witt EM, et al. The Role of Technical Advances in the Adoption and Integration of Patient-Reported Outcomes in Clinical Care. Medical care. 2015; 53(2): 153-159. doi: https: //doi.org/10.1097/MLR.0000000000000289
- Lohr KN, Zebrack BJ. Using patient-reported outcomes in clinical practice: challenges and opportunities. Quality of Life Research. 2008; 18(1): 99-107. doi: https: //doi.org/10.1007/s11136-008-9413-7
- Chang, CH. Patient-reported outcomes measurement and management with innovative methodologies and technologies. Qual Life Res. 2007; 16(Suppl 1): 157-166. https: //doi.org/10.1007/s11136-007-9196-2
- Toogood PA, Abdel MP, Spear JA, Cook SM, Cook DJ, et al. The monitoring of activity at home after total hip arthroplasty. Bone Joint J. 2016; 98-B(11): 1450-1454. doi: 10.1302/0301-620X.98B11.BJJ-2016-0194.R1
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, et al. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics. 2009; 42(2): 377-381. doi: https: //doi.org/10.1016/j.jbi.2008.08.010
- Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics. 2019; 95: 103208. doi: https: //doi.org/10.1016/j.jbi.2019.103208
- Vaughn NH, Dunklebarger MF, Mason MW. Individual Patient-reported Activity Levels Before and After Joint Arthroplasty Are Neither Accurate nor Reproducible. Clin Orthop Relat Res. 2019; 477(3): 536-544. doi: 10.1097/CORR.0000000000000591
- Schmal H, Holsgaard-Larsen A, Izadpanah K, Brønd JC, Madsen CF, et al. Validation of Activity Tracking Procedures in Elderly Patients after Operative Treatment of Proximal Femur Fractures. Rehabil Res Pract. 2018; 2018: 3521271. doi: 10.1155/2018/3521271
- Tophøj KH, Petersen MG, Sæbye C, Baad-Hansen T, Wagner S. Validity and Reliability Evaluation of Four Commercial Activity Trackers’ Step Counting Performance. Telemed J E Health. 2018; 24(9): 669-677. doi: 10.1089/tmj.2017.0264
- Twiggs J, Salmon L, Kolos E, Bogue E, Miles B, et al. Measurement of physical activity in the pre- and early post-operative period after total knee arthroplasty for Osteoarthritis using a Fitbit Flex device. Med Eng Phys. 2018; 51: 31-40. doi: 10.1016/j.medengphy.2017.10.007
- Bini SA, Shah RF, Bendich I, Patterson JT, Hwang KM, et al. Machine Learning Algorithms Can Use Wearable Sensor Data to Accurately Predict Six-Week Patient-Reported Outcome Scores Following Joint Replacement in a Prospective Trial. J Arthroplasty. 2019; 34(10): 2242-2247. doi: 10.1016/j.arth.2019.07.024
- Sharma L, Sinacore J, Daugherty C, et al. Prognostic factors for functional outcome of total knee replacement: a prospective study. J Gerontol A Biol Sci Med Sci. 1996; 51(4): M152-M157. doi: 10.1093/gerona/51a.4.m152 Copy
- Fortin PR, Clarke AE, Joseph L, et al. Outcomes of total hip and knee replacement: preoperative functional status predicts outcomes at six months after surgery. Arthritis Rheum. 1999; 42(8): 1722-1728. doi: 10.1002/1529-0131(199908)42: 8< 1722: : AID-ANR22>3.0.CO; 2-R
- Lingard EA, Katz JN, Wright EA, Sledge CB. Kinemax Outcomes Group. Predicting the outcome of total knee arthroplasty. J Bone Joint Surg Am. 2004; 86(10): 2179-2186. doi: 10.2106/00004623-200410000-00008
- Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. Can Preoperative Patient-reported Outcome Measures Be Used to Predict Meaningful Improvement in Function After TKA?. Clin Orthop Relat Res. 2017; 475(1): 149-157. doi: 10.1007/s11999-016-4770-y
- Fitzgerald JD, Orav EJ, Lee TH, et al. Patient quality of life during the 12 months following joint replacement surgery. Arthritis Rheum. 2004; 51(1): 100-109. doi: 10.1002/art.20090
- Mizner RL, Petterson SC, Snyder-Mackler L. Quadriceps strength and the time course of functional recovery after total knee arthroplasty. J Orthop Sports Phys Ther. 2005; 35(7): 424-436. doi: 10.2519/jospt.2005.35.7.424
- Giesinger JM, Kuster MS, Behrend H, Giesinger K. Association of psychological status and patient-reported physical outcome measures in joint arthroplasty: A lack of divergent validity. Health Qual Life Outcomes. 2013; 11: 64. doi: 10.1186/1477-7525-11-64