Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Prabhakaran A; Stasinou T; Gkentzis Agapios*
*Corresponding Author: Gkentzis Agapios
Consultant Urologist, Bolton Urology Centre, Royal Bolton Hospital, Minerva Road, Farnworth, Bolton BL4 0JR, UK.
Email: agapios.gkentzis@boltonft.nhs.uk
Article Info
Received: Sep 26, 2024
Accepted: Oct 18, 2024
Published: Oct 25, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Agapios G (2024).
Abstract...
Catheterisation is a common urological procedure. Inflation of a urethral catheter balloon inside the ureter is a rare but possible complication of urethral catheterisation. We report two such cases, in view of highlighting warning signs to alert misplacement and share our journey of treating such a complication.
Keywords: Catheterisation; Complication; Misplacement.
Citation: Prabhakaran A, Stasinou T, Agapios G. The Inadvertent Placement of a Urethral Catheter into the Ureter: A Rare but Serious Complication. J Clin Med Surgery. 2024; 4(2): 1169.
Introduction
Urethral catheterisation is a common urological procedure that is often uneventful. A rare, but serious, complication can be the inadvertent placement of a urethral catheter in the ureter. This can often present with abdominal or flank pain, haematuria, or sepsis. Investigations may reveal deteriorating renal function, ureteric obstruction with hydronephrosis, or ureteric injury. We describe two cases encountered in our district general hospital and the sequelae of management, with view to preventing future occurrences.
Case presentations
Case 1
An 88-year-old man, with a background of intermittent small bowel obstruction secondary to hernias and adhesions following surgery for colorectal cancer, on a long- term catheter following his neoadjuvant radiotherapy, had his routine catheter change in hospital following admission under general surgery. He had a small capacity bladder and could normally only tolerate 6 ml of catheter balloon inflation. He complained of abdominal pain five hours post catheter exchange. On examination, the catheter was by passing, the lower abdomen was soft but tender, the bladder was not palpable, his penis was oedematous, and less than 10 ml of urine had drained into the catheter over several hours. The nursing team could not deflate the catheter balloon when they attempted to change it again, and a referral to urology ensued.
A further attempt at deflating, then over inflating the balloon was made. As this was unsuccessful, the patient underwent a flexible cystoscopy, as he could not have a radiological puncture of his urethral catheter balloon, because of his hernias. Cystoscopy revealed a very small bladder capacity, of about 100 ml, and multiple diverticula. A part of the catheter balloon was visualized, presumed to be in a diverticulum, but the catheter tip not seen. An attempt to deflate the balloon with a Botox needle was made, but it was unsuccessful, and the procedure was subsequently abandoned. The next step was to cut the catheter end, including the balloon outlet, allowing the water in the balloon to drain with the assistance of gravity, and a clip placed on the cut end to prevent the catheter from further retracting into the bladder.
A Computerized Tomography (CT) scan of the abdomen and pelvis was performed, revealed that the Foley catheter had been advanced with the balloon inflated half- way up the right ureter (Figure 1). The patient was discovered to have a horseshoe kidney, and the right side was moderately hydronephrotic. Were the balloon not to drain overnight, the patient was consented and booked for a right ureteroscopy and removal of catheter, which if failed, then alternatively he would be for a nephrostomy to happen in-hours the next day. Meanwhile, the patients clinical condition deteriorated rapidly, a DNACPR was put in place, with conservative management of his bowel obstruction proving unsuccessful. The patient was incredibly high risk for operative management, both from a general surgical and urological perspective. Despite his clinical deterioration, and after discussion with the patient and family, we felt it appropriate and, in the patients’ best interest, to proceed with surgery to address his immovable catheter.
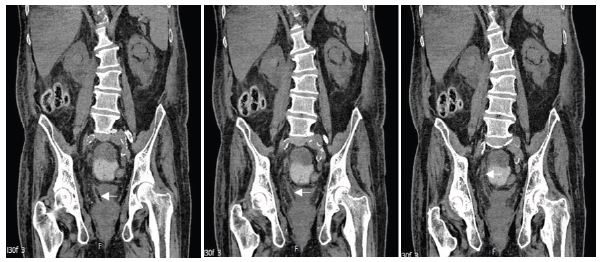
Figure 1: A series of CT images demonstrating the course of the catheter travelling up the right ureter.
A right flexible ureteroscope was passed alongside his catheter and the balloon visualised, fully inflated in the upper ureter. The balloon was burst with a TULA LASER, and catheter was then removed. An 8F/26 JJ stent was inserted with strings on, and a urethral catheter was also inserted, with balloon position confirmed using cystogram, with a post-operative plan to remove the stent in 48 hours. Regardless of the urological success, the patients’ condition worsened in the following days due to the concurrent bowel obstruction, requiring TPN a few days later, and then sadly passed away due to haematemesis nine days after the misplaced catheter was removed.

Figure 2: Retrograde studies performed during right flexible ureteroscopy.
Case 2
A 72-year-old woman, with a background of cerebrovascular accident resulting in left- sided weakness, non-Hodgkin’s lymphoma and a previous pelvic fracture following which she was bedbound and required a long-term catheter, presented to hospital with vomiting, tenderness in the left iliac fossa and raised inflammatory markers. She endured a difficult urethral catheter exchange in the community a few days prior to her admission with the patient experiencing left flank pain during the catheterisation and mild haematuria immediately post insertion.
A CT abdomen and pelvis without contrast revealed a left-sided hydronephrosis and hydroureter down to an obstructive left mid ureteral stone of 7 mm, and a duplex upper pelvicalyceal system. The stone was located approximately 13 cm above the left ureterovesical junction.
The patient was taken for an emergency cystoscopy and left sided retrograde studies and semi-rigid ureteroscopy for removal of the ureteric stone. The patient had a small capacity bladder and a golf-hole type of ureteric orifice but the retrograde ureterogram was inconclusive. It was felt that the distal ureter was chronically dilated. The stone proximally to the dilated distal ureter was removed with endoscopic basket. A ureteric stent was inserted, and this was removed two weeks later. However, the patient had persistent left loin pain and low-grade sepsis. A further repeat contrast urinary CT scan of the abdomen and pelvis demonstrated poor contrast excretion from the persistently hydronephrotic left kidney with evidence of contrast leak from the distal ureter; the patient had developed a collection in the left perivesical space from presumed persistent urinary leak.
The case was discussed in uro-radiology multidisciplinary team meeting, as the cause of the initial pathology was challenging to ascertain, given that the ureteric stone was proximal to the site of the ureteric perforation. As the ureteric orifice was very dilated on the endoscopic assessment and the patient had developed severe pain/haematuria at the time of catheter change in the community we concluded that catheter had inadvertently been inserted in left ureter causing ureteric rupture when the balloon was inflated. Due to the presence of ureteric leak and sepsis we performed a flexible cystoscopy and distal left ureteroscopy with retrograde ureteropyelogram and cystogram and left ureteric stent insertion. The bladder was found to have a small capacity, a dilated opening of the left ureter, florid inflammatory reaction at the area of ureteric perforation with contrast extravasation, however, contrast did also advance to the kidney (Figure 3a). A stent was inserted, and cystogram was used to assess position of the catheter, with evidence of left vesicoureteric reflux, but no further extravasation from minimal distention of bladder. Following this, the patient had an elective left ureteroscopy to ascertain the healing of the distal ureter 2 months later (Figure 3b); there was no further leak; she is currently asymptomatic from the urinary tract and continues to have a long-term catheter.
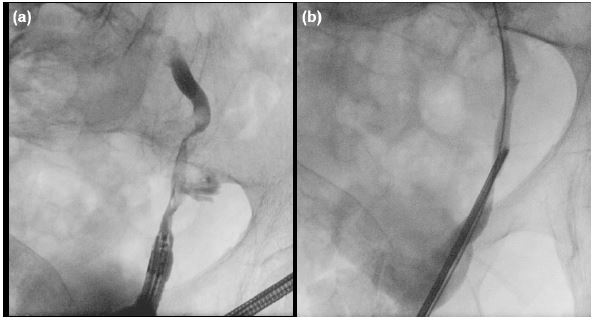
Figure 3: (a) Distal left ureteroscopy demonstrating contrast extravasation and contrast advance into the kidney. (b) Repeat ureteroscopy 2 months later demonstrating healed distal ureteric injury.
Discussion/conclusion
Although rare, urethral catheter misplacement into the ureter can result in serious and devastating consequences for patients. According to existing literature, catheterised patients with a neurogenic bladder are at a higher risk of experiencing this complication [1].
Misplacement of a urethral catheter usually results in pain, which alerts a healthcare practioner to a possible complication with the procedure and trigger corrective action. The loss of this negative feedback is in part responsible for the delayed detection of the misplacement of the urethral catheter in the first case.
The first patient had radiotherapy for his bowel cancer, which resulted in irritative symptoms that meant he struggled to manage his urinary control and led him to having a long-term catheter. Having a catheter in-situ long-term results in bladder contraction [2]. This coupled with the irritative symptoms the patient experienced secondary to his radiotherapy meant that he usually complained of pain during all correctly placed catheter changes and could only tolerate about 6 ml in the balloon. His response during the insertion didn’t serve enough as a warning, and so it was only after urine output reduced were staff inclined to contact the Urology Team.
Additionally, a contracted bladder could result in distorted anatomy of the bladder and the ureteric orifices. Anatomical variance such as a horseshoe kidney for the first patient, and a duplex ureteric system (for the second case would further compound this anatomical distortion [3]. During flexible cystoscopy, both patients were found to have a very small capacity bladder, and ureteric orifices that were very large. This automatically increases the possibility of misplacement of urethral catheter tips into the ureter, when compared to patients with normal anatomy [4].
The lesson to be learnt from the first case is that when dealing with a frail patient with concurrent acute surgical pathology, the sequential progressively more invasive approach to management of a misplaced retained catheter is probably the most ideal. It’s interesting to note that where a needle has failed, a laser fibre has succeeded in puncturing the catheter balloon and enabling removal of the catheter.
Although there was no image confirming a catheter balloon as a cause of the ureteric rupture in the second case, we were perplexed by the presentation and the anatomy demonstrated on the images. Usually, an obstructing ureteric stone results in renal calyceal rupture as that is the weakest point in the urinary system [5]. It was unusual for the rupture site in the ureter to be distal to the stone. We then supposed that perhaps because the patient had a small bladder capacity, and large ureteric orifices which would be subject to refluxing of urine, this could have put pressure and resulted in a perforation closer to the vesicoureteric junction. What didn’t quite fit with this theory was that the ureter distal to the stone was not dilated. A distance of about 5-6 cm was present between the site of the obstructing stone and site of the ureteric tear, and so the most plausible explanation was that during insertion of the urethral catheter, the catheter had inadvertently travelled up the ureter and resulted in a perforation.
Rare complications of common procedures are often forgotten until serious harm results. We presented these two cases with the aim of highlighting potential overlooked risk factors that should automatically alert us to error, and trigger action in order to promote patient safety. We hope to add to the small but growing body of evidence that urethral catheterisation in patients with a long-term catheter is a slightly more complex affair than might be previously supposed.
References
- Luo R, Lee SL, Ng FC, Koh LT. Inadvertent placement of a urinary catheter into the ureter: A report of 3 cases and review of the literature. Asian J Urol. 2017; 4: 256-261.
- Panwar VK, Tosh JM, Mittal A, Narain TA, Mandal AK, et al. Small contracted bladders posing bigger problems: Etiology, presentation, and management and a short review of literature. J Family Med Prim Care. 2022; 11: 2246-2251.
- Cascio S, Sweeney B, Granata C, Piaggio G, Jasonni V, et al. Vesicoureteral reflux and ureteropelvic junction obstruction in children with horseshoe kidney: treatment and outcome. Journal of Urology. 2002; 167: 2566-2568.
- Kato H. Incorrect positioning of an indwelling urethral catheter in the ureter. International Journal of Urology. 1997; 4: 417-418.
- Kheiri B, Kazmi I, Madala S, Abu Sitta E. From a stone to rupture: Calyceal rupture secondary to obstructive uropathy. Clinical Case Report. 2018; 25: 191-1192.