Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Giulia Scopetani*; Matthias Kirsch
*Corresponding Author: Giulia Scopetani
Department of Cardiovascular Surgery, CHUV, Vaudois University Hospital Center, Lausanne, Switzerland.
Tel: +41-79-55-65-457;
Email: giulia.scopetani@chuv.ch
Article Info
Received: Sep 24, 2024
Accepted: Oct 16, 2024
Published: Oct 23, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Scopetani G (2024).
Abstract...
Background: Sinus of Valsalva Aneurysm (SVA) is a rare heart defect resulting from the frailty of the elastic lamina of the aorta. SVA can be congenital or acquired and most often, it concerns the right SV.
Methods: We describe the case of a 61-year-old male patient referred to our hospital for elective aneurysm repair of the right coronary sinus of Valsalva.
Results: Endoluminal inspection highlighted an aneurysm originating in the right coronary sinus, laminating the origin of the right coronary artery. Intraoperatively, the complex asymmetric anatomy, jointly with the poor quality of the native cusps, conducted us to perform a modified Bentall procedure.
Conclusion: Isolated SVA is a rare condition. Although the optimal management for the unruptured SVA is debated, early surgical intervention is suggested due to a potential intra or extra-cardiac rupture. Different surgical approaches were described. We believe the modified Bentall procedure is safe and durable in marked eccentric aortic regurgitation cases and with a highly deformed root.
Keywords: Aortic root; Sinus of valsalva aneurysm; Modified bentall procedure; Right coronary sinus.
Citation: Scopetani G, Kirsch M. How to Treat Unruptured Sinus of Valsalva Aneurysm: A Review of the Literature. J Clin Med Surgery. 2024; 4(2): 1168.
Introduction
The Sinus of the Valsalva Aneurysm (SVA) is an infrequent cardiac anomaly, a product of the frailty of the elastic lamina at the junction of the aortic media and the annulus fibrosus.
SVA can be congenital or acquired. When congenital, SVA is often associated with Marfan syndrome or other connective tissue diseases. Moreover, it is usually associated with other cardiac anomalies, including doubly committed juxta-arterial ventricular septal, perimembranous ventricular septal defect, coronary anomalies, bicuspid aortic valve, aortic regurgitation, pulmonary stenosis, tetralogy of Fallot, coarctation of the aorta or atrial septal defect. Acquired forms of SVA are associated with infections (syphilis, bacterial endocarditis, and tuberculosis), systemic inflammatory diseases (Behçet disease, ankylosing spondylitis, Takayasu disease), connective tissue disorders (systemic lupus erythematosus), medial cystic necrosis, traumatic and degenerative diseases (atherosclerosis), strenuous physical activity and abuse of drugs or alcoholism [1,2]. SVAs are more frequently in men (4:1). The incidence is higher in the Asian populations, where a ruptured SVA is a simple and invariant disease entity, in contrast to the more diverse and protean disease profiles found in the Western series [3,4]. The incidence of unruptured SVA is around five times higher in Asians than in Westerners. The actual prevalence is unknown; the estimated rate is approximately 0.09% of the general population up to 3.5% of all congenital cardiac defects [5].
SVA most often affects one of the SVs and originates predominantly from the right SV (70% of cases) and non-coronary Sinus in 25% [6-9]. Unruptured SVAs present at a median age of 59 years.
While ruptured SVAs are an emergency, the management of unruptured SVAs remains contentious despite early surgical intervention being recommended due to life-threatening complications. At present, the patient will be operated on according to the most recent guidelines regarding ascending aortic aneurysm [10].
Case report
A 61-year-old male patient was referred to our hospital for elective aortic root surgery. He had been observed by his general practitioner for years for an aneurysm of the right coronary sinus of Valsalva and had already refused surgery. The medical history is notable for arterial hypertension, alcoholism, active smoking and ex-drug addiction. The patient experienced only intermittent palpitations and was otherwise asymptomatic. The electrocardiogram showed an ectopic atrial rhythm. During the preprocedural diagnostic work-up, Transthoracic Echocardiography (TTE) was performed. It revealed a dilated Left Ventricle (LVESD 59 mm) with a LVEF at 54%, a tricuspid aortic valve with moderate regurgitation and an aortic root measured at 62 mm. A subsequent cardiac CT scan proved the diagnosis of isolated aneurysmal dilatation of the right coronary sinus, measured up to 65 mm, with the other two sinuses also dilated at 43 and 45 mm, with a normal sino-tubular junction (Figure 1). Intraoperatively, endoluminal inspection highlights this aneurysm developed in the right coronary sinus, laminating the origin of the right coronary artery. The right coronary and the conus artery originated from the edge of the aneurysm and have been carefully separated from the dilated sinus. The complex asymmetric anatomy, together with the inadequate quality of the native cusps, led us to perform a modified Bentall procedure with a 25 mm frameless porcine bioprosthesis (Medtronic Freestyle). Pledgeted 4/0 polypropylene traction sutures are placed at each aortic valve commissure, and the valve leaflets are excised, leaving a slight edge. The coronary arteries were isolated with a small button of the full-thickness aortic wall. The Freestyle bioprothesis was fixed in the outflow chamber of the left ventricle. The left coronary artery was reimplanted, then the right one, in the respective ostia of the bioprosthesis, with a continuous 5/0 polypropylene suture. Then, the aortic graft is trimmed to a suitable distance and sutured to the native ascending aorta using a 4/0 continuous polypropylene suture. Weaning from CPB was obtained in excellent conditions. (CPB time: 74 minutes, Cross clamp time: 59 minutes). The postoperative course was characterized by a right anterior junctional ischemic stroke, with a complete resolution of neurological disorders after the introduction of Clopidogrel.
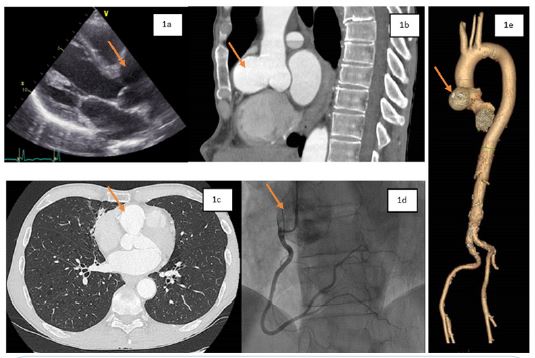
Figure 1: The aneurismal dilatation of the right coronary sinus (arrow) on TEE at parasternal long axis view (1a); (1b). Sagittal plan of the cardiac CT (arrow on the right coronary sinus); (1c). Axial plan of the cardiac CT (arrow on the right coronary sinus); (1d). Right coronary artery with view of the right sinus of Valsalva (arrow) on coronary angiography; (1e). Three-dimensional CT displaying the aneurysm (arrow).
Table 1: Demographic, clinical presentation, treatment approaches and outcomes of sinus of valsalva aneurysm.
| Reference | Year | Sex | Age | Sinus of origin | Type of Surgery | Emergency Surgery | Particularities |
|---|---|---|---|---|---|---|---|
| Farì G et al. | 2020 | M | 58 | R | None | Yes | Post mortem |
| Lahrouchi N et al. | 2014 | M | 14 | R | Pericardial patch | No | Down’s Syndrome |
| Doost A et al. | 2020 | M | 24 | R | Pericardial patch | Yes | |
| Weinreich M et al. | 2015 | M | 76 | R | A valve-sparing aortic root replacement | No | |
| Weinreich M et al. | 2015 | F | 54 | NC | A valve-sparing aortic root replacement | No | |
| Miklos P et al. | 2020 | M | 68 | R | A remodeling technique, with a stabilization of the aortic valveannulus via running suture annu- loplasty | No | |
| Serban AM et al. | 2019 | M | 49 | R | A tubular Dacron prosthèsis; theproximal section of the tubulargraft was tailored to recreate the ex- cised right coronary sinus RCA wasbypassed with a saphenous graft | No | |
| Abetti A et al. | 2020 | M | 47 | R | Pericardial patch | Yes | |
| Li X et al. | 2021 | M | 27 | L | Bentall procedure with a mechanical valve | Yes | Quadricuspid aorticvalve; T. pallidum |
| Wang B et al. | 2019 | M | 46 | NC | Pericardial patch | No | |
| Umeda H etal. | 2018 | F | 69 | R | Gore-Tex patch | No | |
| Qian H etal. | 2016 | F | 60 | L | Reconstruction of the coronary arteries | No | |
| Ponti A et al. | 2017 | M | 71 | L | Dacron patch | No | |
| Luo Y etal. | 2017 | M | 48 | NC | Bentall procedure | No | |
| Guner A et al. | 2017 | M | 45 | R | Cabrol's technique | No | |
| Gong W et al. | 2015 | M | 45 | L andR | Aortic valve annuloplasty, aortic sinus repairand coronary arteryostia graft | No | |
| Karvounaris S etal. | 2015 | F | 63 | L | None | Yes | Obstruction of left coronary flow, ischaemicheart failure and the ongoing myocardial infarction, which led to the patient’s unfavourable outcome |
| Ma L etal. | 2022 | M | 51 | R | Bovine epicardial patch | Yes | |
| P Ramirez-Rangeb et al. | 2022 | M | 34 | R | Percutaneous closure | Yes | |
| Petersen J et al. | 2022 | M | 57 | R | Bovine pericardial patch | No |
Discussion
The isolated Sinus of the Valsalva aneurysm is a rare condi- tion. In a recent review of the literature, Nguyen et al. proved that patients with unruptured SVA could be asymptomatic (9%) or present with non-specific symptoms [11-17]. Arrhythmias and conduction abnormalities are common in patients with un- ruptured SVAs (atrial fibrillation (9%), sinus tachycardia (4%), sinus bradycardia (2%) [18]. Comorbidities include hyperten- sion (19%), obstructive sleep apnea (2%), smoking (8%), dys- lipidemia (2%) and type II diabetes (2%) [19]. The presence of the aneurysm can cause valvular regurgitation, annular dilation or deformity, and compression of the coronary arteries, cardi- ac chambers and outflow tracts [20-21]. Rupture often arises from a right sinus aneurysm swelling into the right ventricle, followed by a noncoronary sinus aneurysm rupturing into the right atrium [21]. In our patient, it is difficult to establish wheth- er the aneurysm is congenital or acquired, related to the use of drugs and alcohol, and after excluding potential congenital causes. The strategy was to repair the aortic root by excision of the aneurysmal sinus with or without the aid of a pericardial patch, especially given the relatively young age of the patient and the history of drug abuse, with the risk of recurrence and, therefore, an increased risk of endocarditis with a prosthetic valve. Valve-sparing procedures (reimplantation or remodeling) could also be an option, but not in marked aortic root asym- metry cases. We could not maintain the native valve, given the marked asymmetry of the aortic root and the moderate regur- gitation. In a tricuspid aortic valve with root aneurysms (root phenotype), surgery should be considered when the maximum aortic diameter is 50 mm, as recommended in recent guidelines [10]. Although optimal management for the unrupted SVA is not defined, early surgical intervention is recommended due to a potential intra or extra-cardiac rupture. Isolated SVA should be treated by surgery as soon as possible after diagnosis since they are life-threatening circumstances. Further surgical ap- proaches were described (Table 1). The surgical strategy can be a primary closure of the aneurysm, patch repair or aortic root replacement with or without valve replacement. Direct closure may aggravate aortic regurgitation by distorting the aortic an- nulus and may be accountable for the recurrences. Aortic valve replacement or valvuloplasty may be necessary for aortic valve regurgitation. The long-term results of surgical repair are excellent. Percutaneous treatment of an aneurysm of the Sinus of Valsalva is, in some instances, also feasible in children [22]. Aor- tic valve replacement is usually performed if concomitant aortic regurgitation is present [23,24].
Conclusion
Isolated SVA is a rare condition, and various surgical treat- ments have been described. The modified Bentall procedure is a secure and practical option in case of significant eccentric aor- tic regurgitation and with an extremely deformed root.
Abbrevations: CPB: CardioPulmonary bypass; CT: Computed Tomography; LVEF: left Ventricular Systolic Function; LVESD: Left Ventricular End-Systolic Diameter; SV: Sinus of Valsalva; SVA: Sinus of Valsalva Aneurysm; TTE: TransThoracic Echocardiogra- phy.
Declarations
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical statement: Patient consent was obtained.
Conflict of interest statement: Authors have nothing to dis- close about commercial support.
Data avaibility statement: There are no new data associated with this article.
References
- Fari G, Pennacchia I, Stigliano E, Oliva A, et al. Right sinus of Valsalva aneurysm. Cardiovascular Pathology. 2020; 47: 107209.
- Lahrouchi N, Rammeloo LA, Koolbergen DR, et al. Ruptured aneurysm of the right coronary sinus of Valsalva in a child with Down syndrome. Cardiology in the Young. 2014; 24: 376-378.
- Doost A, Craig JA, Soh SY. Acute rupture of a sinus of Valsalva aneurysm into the right atrium: a case report and a narrative review. BMC Cardiovasc Disord. 2020; 20(1): 84.
- Chu SH, Hung CR, How SS, et al. Ruptured aneurysms of the sinus of Valsalva in Oriental patients. J Thorac Cardiovasc Surg. 1990; 99(2):288-98.
- Weinreich M, Yu PJ, Trost B. Sinus of Valsalva Aneurysms Review of the Literature and an Update on Management. Clin Cardiol. 2015; 38: 185-9.
- Pólos M, Sulea CM, Benke K, et al. Giant unruptured sinus of Valsalva aneurysm successfully managed with valve-sparing procedure- a case report. J Cardiothorac Surg. 2020; 15: 6.
- Serban AM, Bätrâna N, Cocoi M, et al. The role of echocardiography in the diagnosis and management of a giant unruptured sinus of Valsalva aneurysm. Med Ultrason. 2019; 21: 194-6.
- Abetti A, Gandet T, Amri AA, et al. Ruptured right Valsalva sinus into the right atrium due to infective endocarditis: a case report. Pan Afr Med J. 2020; 37: 65.
- Li X, Zhong Y, Rao L, et al. A dissecting aneurysm of the sinus of Valsalva involving the inter-ventricular septum in a patient with syphilis and a quadricuspid aortic valve. Echocardiography. 2021; 38: 1061-3. doi: 10.1111/echo.15055
- Czerny M, Grabenwöger M, Berger T, et al. EACTS/STS Scientific Document Group. EACTS/STS Guidelines for diagnosing and treating acute and chronic syndromes of the aortic organ. Eur J Cardiothorac Surg. 2024; 65(2): ezad426.
- Wang B, Ma D, Qu L, et al. Sinus of Valsalva aneurysm protruding into the mitral anterior leaflet causing dyspnea: A CARE-compliant case report. Medicine (Baltimore). 2019; 98: 18169.
- Umeda H, Isotani A, Arita T, et al. Rapid growth of thrombus formation in the unruptured sinus of Valsalva aneurysm following coronary angiography. J Echocardiography. 2018; 16: 182-4.
- Qian H, Ouyang Q, Li Y, et al. Compression of left ventricle by a rare giant unruptured sinus of Valsalva aneurysm. Anatol J Cardiol. 2016; 16: 1-2.
- Ponti A, Qanadli SD, Kirsch M, et al. Left sinus of Valsalva aneurysm as a cause of chronic stable angina. Interact Cardiovasc Thorac Surg. 2017; 24: 967-8.
- Luo Y, Fang Z, Meng W. A giant aneurysm of noncoronary sinus of Valsalva concomitant with aortic regurgitation and mitral regurgitation. Echocardiography. 2017; 34: 796-8.
- Guner A, Celik M, Kahyaoglu M, et al. Multiple aneurysmatic involvement of sinus of Valsalva. Echocardiography. 2017; 34: 627-8.
- Nguyen Q, Vervoort D, Phan K, et al. Surgical management for unruptured sinus of Valsalva aneurysms: a narrative review of the literature. J Thorac Dis. 2021; 13(3): 1833-1850.
- Gong W, Ye X, Wang Z, et al. Two balls around aortic root: Multiple huge unruptured aneurysms of the Valsalva sinus. Eur Heart J Cardiovasc Imaging. 2015; 16: 827.
- Xu B, Kocyigit D, Betancor J, et al. Sinus of Valsalva Aneurysms: A State-of-the-Art. Imaging Review. J Am Soc Echocardiography. 2020; 33: 295-312.
- Karvounaris S, Michas G, Karampetsos V, et al. Giant Unruptured Left Sinus of Valsalva Aneurysm as an Unusual Cause of Ischemic Heart Failure. Hellenic I Cardiol. 2015: 56: 441-3.
- Ma L, Yang J, Liu Y, et al. Case report: Acute ST-elevation myocardial infarction and cardiogenic shock caused by a giant right sinus of Valsalva aneurysm and right coronary artery compression. Front. Cardiovasc. Med. 2022; 9: 1013044.
- Ramirez-Range P, Garcia-Cruz E, Fritche-Salazar JF, et al. Percutaneous closure of a ruptured right coronary sinus of Valsalva aneurysm that mimics severe aortic regurgitation. Echocardiography. 2022; 39: 1138-1141.
- Lin Y, Yin K, Wang Y, et al. Sinus of Valsalva aneurysms with concomitant aortic insufficiency: how should the aortic valve be managed? Interact Cardiovasc Thorac Surg. 2018; 26(2): 210-5.
- Petersen J, Holst T, Pecha S, et al. Sinus of Valsalva Aneurysm Treated by Aortic Valve Reimplantation Technique. Braz J Cardiovasc Surg. 2022; 37(6): 949-951.