Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Samantha A Cintron1*; Francisco Diaz2; Qiuhua Shen1; Frances M Yang1; Branden Comfort3; Janet D Pierce1
*Corresponding Author: Samantha A Cintron
School of Nursing, University of Kansas Medical Center, Mail Stop 4043, Kansas City, KS 66160, USA.
Tel: (785) 766-6827, Fax: (913) 588-1660;
Email: sjohnson18@kumc.edu
Article Info
Received: Sep 19, 2024
Accepted: Oct 04, 2024
Published: Oct 11, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Cintron SA (2024).
Abstract...
Objective: One possible treatment for post-COVID-19 conditions is a mushroom supplement called Active Hexose Correlated Compound (AHCC). The purpose was to determine if taking AHCC twice a day for 30 days decreases symptoms and improves physiological functions in these patients.
Methods: Twelve patients with post-COVID-19 conditions completed three PROMIS® questionnaires (fatigue, dyspnea, cognitive function), pulmonary testing (exhaled nitric oxide and pulmonary function testing), and a blood draw to evaluate natural killer cells and mitochondrial membrane potential before and after 30 days of consuming the mushroom supplement. Differences between the pre- and post-variables were calculated using a Wilcoxon signed-rank test.
Results: Symptom measures improved significantly, with a reduction in fatigue from 46.5 [95% CI, (39.66, 53.34)] to 32.08 [(24.2, 39.97); p=0.0024] and dyspnea from 17.5 [95% CI, (8.383, 26.62)] to 12.75 [(5.837, 19.66); p=0.0273]; and increase in cognitive function from 51.25 [95% CI, (38.46, 64.04)] to 71.83 [(61.63, 82.03); p=0.0127]. Forced vital capacity significantly improved from 3.794 L [95% CI, (3.036, 4.552)] to 3.89 L [(3.151, 4.629); p=0.0425]. Consuming AHCC for 30 days resulted in a significant decrease in the number of natural killer cells (CD14-/CD56+ and CD16+/CD56+; both at p=0.007) and improved mitochondrial membrane function (19557.11 [95% CI, (11606.39, 27507.84)] to 38990.67 [(28919.21, 46839.90); p=0.0280]).
Conclusion: Our results suggest that AHCC reduces symptoms and improves physiologic functions in patients suffering from post-COVID-19 conditions, however these findings should be investigated in a larger clinical trial.
Keywords: Mitochondrial health; Natural killer cells; Patient-reported outcome; Post-COVID-19 conditions.
Citation: Cintron SA, Diaz F, Shen Q, Yang FM, Comfort B, et al. Reducing symptoms and improving physiological functions in patients with post-covid-19 conditions using a mushroom supplement: A pilot study. J Clin Med Surgery. 2024; 4(2): 1167
Introduction
A multitude of long-lasting symptoms have been described after the start of the coronavirus disease 2019 (COVID-19) pandemic. Many terms and definitions have been utilized to describe these persistent symptoms. These new, recurring, or continuing health problems at least 4 weeks after the initial COVID-19 infection have been termed post-COVID-19 conditions [1]. While the exact prevalence rate is unknown, post-COVID-19 conditions have been estimated to impact 10% [2] to 43% [3] of individuals infected with COVID-19 worldwide and continue to impact quality of life. Many treatments for post-COVID-19 conditions focus on symptom management, and no broadly effective treatments have been identified. Therefore, investigating a treatment based on the underlying pathophysiologic mechanisms could help reduce or eliminate the symptom burden of individuals suffering from post-COVID-19 conditions.
The pathophysiologic mechanisms underlying post-COVID-19 conditions are unclear, but many hypotheses and studies suggest the mechanisms of action. Some of these mechanisms include cellular alterations directly caused by the virus [2-4], dysregulated immune function [5,6], and impaired cellular bioenergetics [7,8]. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus uses the Angiotensin-Converting Enzyme 2 (ACE2) receptor for cell entry though activation of its spike protein [9]. These ACE2 receptors are found in many cell types and tissues including the lungs, blood vessels, heart, liver, and gastrointestinal track. These organs were identified as more impaired in individuals with post-COVID-19 conditions than in healthy controls [10]. Chronic inflammation has also been proposed as a mechanism resulting in organ dysfunction [11]. Singh, Chaubey, Chen and Suravajhala [12] hypothesized that SARS-CoV-2 viral RNA can invade the mitochondria resulting in mitochondrial dysfunction, inflammation, and impaired immune response. Utilizing antioxidants has been proposed as a treatment to improve mitochondrial function, reduce oxidative stress, and help replenish T cells [13].
Active hexose correlated compound (AHCC) is an over-the-counter supplement derived from the mycelia of shiitake mushrooms (Lentinus edodes) [14]. AHCC is rich in alpha-1,4-glucan oligosaccharides, which are believed to enhance its biologic activities and promote white blood cell production [15-17]. Specifically, studies have found that AHCC has increased the number and activity of dendritic cells, [18] enhanced cytokine production, increased optimal Natural Killer (NK) cell activity, promoted macrophage and T-cell activity [16-20], and reduced fatigue [21]. The AHCC supplement has been shown to modulate the immune system in human papillomavirus [16,22] and influenza [23]. In addition, AHCC has antioxidant properties and attenuates oxidative stress [24]. Therefore, in this study our aim was to determine if AHCC improves physiological (mitochondrial, immune, and pulmonary) functions and decreases symptoms in patients with post-COVID-19 conditions.
Material and methods
This pilot study was designed to determine the effects of AHCC on physiological functions and symptoms in patients with post-COVID-19 conditions. The study population consisted of 12 COVID-19 patients who still had symptoms 30 days or more after they were first infected. All participants were asked to come to a Clinical Translational Science Unit between 0700 and 1300 Monday thru Friday to collect all data so that the blood samples could be processed in the afternoon.
Study settings and participants
Patients who participated in this study were recruited from the Internal Medicine clinic of The University of Kansas Health System between August 2022 and December 2022. Consecutive sampling was used until the sample size was met. The inclusion criteria for the study were: (1) adult patients ≥18 years of age; (2) still having symptoms of COVID-19 such as dyspnea, fatigue, or cognitive dysfunction more than 4 weeks after the diagnosis of COVID-19; (3) current symptoms of fatigue, dyspnea, and/or cognitive dysfunction that were a result of contracting COVID-19. Patients were excluded from the study if they were: (1) sensitive or allergic to mushrooms; (2) diagnosed with an autoimmune disease such as multiple sclerosis, systemic lupus erythematosus, or rheumatoid arthritis; (3) currently receiving any cancer treatment; (4) currently taking cytochrome P450 2D6 (CYP2D6) medications. This study was approved by the Institutional Review Board at the University of Kansas Medical Center and exempted from registration. A written informed consent was obtained from all subjects at the beginning of the initial visit.
Intervention
In order to enroll 12 subjects in the study, we attempted to contact 34 individuals being seen in the clinic for post-COVID-19 conditions. Of those 34 individuals, two individuals were no longer having symptoms, two individuals were unable to be contacted after scheduling the appointment, and others did not respond or declined participation. After the initial visit where baseline measures were assessed, participants consumed two mushroom supplements 1 hour before breakfast and at bedtime for a total dose of 3 g/day for 30 days.
PROMIS measures
All participants completed three questionnaires before and after taking AHCC: the National Institutes of Health (NIH) PROMIS® (Patient-Reported Outcomes Measurement Information System) [25] for fatigue (Short Form 13a FACIT-Fatigue v1.0) [26,27], dyspnea characteristics (v1.0) [28], and cognitive function abilities subset (v2.0) [29]. These questionnaires were selected through recommendations from the Epic PROMIS Collaborative to utilize fatigue and dyspnea questions for measuring symptoms of COVID-19 [30] and post-COVID-19 [31] and through consensus among investigators regarding the top three symptoms most often reported by patients with post-COVID-19 conditions.
Pulmonary measures
We completed two noninvasive pulmonary function tests with each participant. For the first test, we used a Fleisch pneumotachograph instrument (Vitalograph®, Lenexa, Kansas, USA) with a disposal filter to measure Forced Vital Capacity (FVC). Next, we measured forced expiratory volume in 1 second (FEV1), and the FEV1/FVC ratio was calculated. This test was completed three times, and the values were averaged. The second measurement was a test of Fractional exhaled Nitric Oxide (FeNO) using an instrument called NIOX® (Circassia Inc., Morrisville, North Carolina, USA). We used the FeNO as an objective measure of airway inflammation.
Immunologic measures
Human NK cells were assessed quantitatively using flow cytometry. Seven milliliters of whole blood were collected from participants via venipuncture in a purple top BD Vacutainer® blood collection tube with Ethylenediaminetetraacetic Acid (EDTA) before and after consuming the mushroom supplement for 30 days.
A five-color panel of antibodies was used to differentiate clusters: CD3, CD56, CD16, CD14, and CD20, with the corresponding fluorescent dyes FITC, PE, and PE-Cy7 (BD Biosciences, USA). During sample preparation, cells were washed with Phosphate Buffer (PBS) followed by addition of the monoclonal antibodies. Staining was run at 25°C in the dark for 15 minutes. After staining, cells were washed twice with PBS. Specimens were analyzed using a flow cytometer (5 laser Aurora, Cytek Biosciences, Fremont, CA, USA) with FlowJo (BD Biosciences, San Jose, CA, USA) software gated for human NK cells. These NK cells were defined using CD3, CD56, CD16, CD14 and CD20. The B cells and macrophages were excluded using CD14 and CD20.
Mitochondrial measure
Another 7 milliliters of whole blood were collected from participants via venipuncture in a yellow top BD Vacutainer® blood collection tube with citrate dextrose before and after consuming the mushroom supplement for 30 days. Lymphocytes were isolated using Accuspin tubes, histopaque 1077, and differential centrifugation. Approximately 2 million lymphocytes were stained with Tetramethylrhodamine Ethyl Ester (TMRE) for mitochondrial membrane potential [32,33]. TMRE is a red-orange color that is cell permeable and positively charged. After isolation of lymphocytes, they were incubated with 10 ng TMRE for 30 minutes at 37°C/5% CO2 in Hanks Balanced Salt Solution (HBSS with Ca2+/Mg2+). TMRE stained cells were washed with HBSS and diluted for flow cytometry analysis. Fluorescent cells were identified and quantified using flow cytometry. Figure 1 illustrates how damaged or depolarized mitochondria from the SARS-CoV2 are unable to retain the TMRE dye due to decreased membrane potential resulting in low fluorescence signals.
Data analysis
Data analyses were conducted with the statistical packages Stata (StataCorp LLC, College Station, TX) and SAS (SAS Institute Inc., Cary, NC). Descriptive statistics were used to characterize the study sample (age, sex, race/ethnicity, and symptoms) and report clinical outcomes (PROMIS questionnaires, mitochondrial membrane, NK, and pulmonary function). Changes in all the physiologic measures from baseline to 30 days were computed for each patient. A nonparametric Wilcoxon signed-rank test was used for all measures to decide whether or not there were significant changes at a 0.05 significance level (Table 1).
Results
A total of 12 participants were enrolled, and the participants completed the pre-post PROMIS questionnaires, pulmonary function tests, blood sampling for NK, and mitochondrial analysis. The age of the patients ranged from 31 to 64 years, and the median age was 52.5. Of the study sample, 10 (83.3%) self-identified as female and 2 (16.7%) as males. All participants self-identified as White and 10 (83.3%) were vaccinated for COVID-19. Each participant consumed at least 80% of the mushroom supplement as evidenced by the remaining number of pills left in the bottle and verbal confirmation.
As shown in Table 1, all symptom measures significantly improved after consuming the mushroom supplement for 30 days. The mean PROMIS fatigue measure was significantly reduced from 46.5 [95% CI, (39.66, 53.34)] to 32.08 [(24.2, 39.97); p=0.0024]. The mean PROMIS dyspnea measure was significantly reduced from 17.5 [95% CI, (8.383, 26.62)] to 12.75 [(5.837, 19.66); p=0.0273]. The mean PROMISE cognition measure increased significantly from 51.25 [95% CI, (38.46, 64.04)] to 71.83 [(61.63, 82.03); p=0.0127], demonstrating reduced brain fog.
We did not find evidence that consuming AHCC for 30 days improved nitric oxide (FeNO), FEV1, or the FEV1/FVC ratio. Forced vital capacity significantly improved from 3.794 L [95% CI, (3.036, 4.552)] to 3.89 L [ (3.151, 4.629); p=0.0425]. The FEV1/FVC ratio decreased significantly from 0.7537 [95% CI, (0.6933, 0.8141)] to 0.7248 [(0.6583, 0.7911); p=0.0425], although this was likely due to no change in FEV1 and increase in FVC.
Levels of NK cells, as measured by CD56+ and CD14- cells, decreased significantly from 47.68 [95% CI, (36.4, 58.96)] to 33.41 [(25.18, 41.64); p=0.0488] after taking the mushroom supplement for 30 days. Figure 2 displays the gating strategy used on the samples. Mitochondrial membrane significantly improved, with TMRE increasing from 19,557.11 [95% CI, (11606.39, 27507.84)] to 38,990.67 [(28919.21, 46839.90); p=0.0280]. No adverse events were reported by participants.
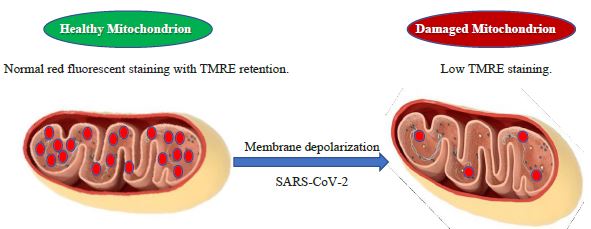
Figure 1: Mitochondrial membrane and TMRE.
SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2;
TMRE: Tetramethylrhodamine Ethyl Ester.
SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2;
TMRE: Tetramethylrhodamine Ethyl Ester.
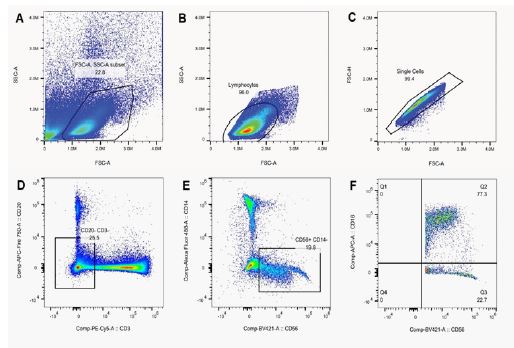
Figure 2: Flow cytometry gating strategy for natural killer cells. (A) Side Scatter (SSC-A) versus forward scatter (FSC-A). (B) Identifying lymphocytes. (C): Gating out doublets. (D): Gated on CD20-/CD3-. (E): Gated on CD14-/CD56+. (F): Gated on CD16+/CD56+. SSC: Side Scatter; FSC: Forward Scatter; A: Area; H: Height.
Table 1: Differences in PROMIS questionnaires and physiological variables before and after consuming a mushroom supplement for 30 days in 12 patients with post-COVID-19 conditions.
| Variable | Mean before | 95%CI before | Mean after | 95%CI after | P-valuea |
|---|---|---|---|---|---|
| PROMIS Fatigue | 46.5 | (39.66, 53.34) | 32.08 | (24.2, 39.97) | 0.0024 |
| PROMIS Dyspnea | 17.5 | (8.383, 26.62) | 12.75 | (5.837, 19.66) | 0.0273 |
| PROMIS Cognition | 51.25 | (38.46, 64.04) | 71.83 | (61.63, 82.03) | 0.0127 |
| Nitric oxide (FeNO) | 21.94 | (18.17, 25.71) | 20.97 | (16.65, 25.29) | 0.5693 |
| FEV1 (L) | 2.869 | (2.252, 3.486) | 2.814 | (2.191, 3.438) | 0.2036 |
| FVC (L) | 3.794 | (3.036, 4.552) | 3.89 | (3.151, 4.629) | 0.0425 |
| FEV1/FVC ratio | 0.7537 | (0.6933, 0.8141) | 0.7247 | (0.6583, 0.7911) | 0.0132 |
| CD14-/CD56+ (cells/mL) | 187297.18 | (26708.86, 347885.50) | 48985.07 | (11178.98, 86791.16) | 0.0070b |
| CD16+/CD56+ (cells/mL) | 174311.63 | (22439.21, 326184.05) | 31163.94 | (5438.32, 56889.56) | 0.0070b |
| TMRE (mV) | 19557.11 | (11606.39, 27507.84) | 38990.67 | (28919.21, 46839.90) | 0.0280c |
aTwo-tailed p-value from a paired-sample Wilcoxon exact test testing change. bSubjects 5, 7 were not included in the NK measures; subject 5 did not provide the after-treatment measure. Subjects 7 was excluded as the cell count datum was an extreme outlier. cSubjects 6, 7, 11 were not included in the TMRE test as there was no staining on subject 11 premeasurement and subject 6 post measurement. Subject 7 was excluded as the datum was an extreme outlier.
FEV1: Forced Expiratory Volume in 1 second; FVC: Forced Vital Capacity; L: Liter; mL: Milliliter; mV: Millivolts; TMRE: Tetramethylrhodamine ethyl ester.
Discussion
The AHCC mushroom supplement has been shown to be effective and safe in reducing viral load and symptoms in influenza, human papilloma virus, and other opportunistic infections [22,23,34,35]. AHCC has also improved the prognosis and chemotherapy-associated adverse effects in patients with cancers [36-38]. Findings from the present study demonstrate a reduction in symptoms and significant changes in NK cell activity and mitochondrial membrane after patients with post-COVID-19 conditions consumed two AHCC supplements twice a day for a total dose of 3 g/day for 30 days. As with other reports [21], patients from this study stated the supplement was easy to take and denied any adverse effects.
A significant reduction in the symptoms of fatigue, dyspnea, and brain fog were seen in the PROMIS measures. These three symptoms were selected based on the literature of the top symptoms seen in post-COVID-19 conditions [39,40]. However, over 200 symptoms that affect nearly every organ system have been reported with post-COVID-19 conditions [41] and research identifying how AHCC impacts other symptoms of post-COVID-19 conditions is needed. There is also some evidence that different variants of COVID-19 cause different symptoms [42]. Therefore, further understanding the pathophysiologic mechanisms of post-COVID-19 conditions and AHCC will be beneficial for targeted treatment.
While patients had a decrease in the PROMIS dyspnea score, patients did not report dyspnea as a primary symptom. Thus, the physiologic pulmonary measures may respond to AHCC in a cohort with worse baseline pulmonary function. For example, the AHCC could modulate the Type 2 inflammation that may be present in the airways of patients with post-COVID-19 conditions. In Type 2 inflammation, Interleukins (IL) such as IL-4 and IL-13 upregulate the activity of the iNOS (inducible nitric oxide synthase) enzyme, which produces NO in the airway. Therefore, AHCC should be tested in patients with post-COVID-19 conditions with severe dyspnea to determine if AHCC has different effects in this specific phenotype of patients.
Natural killer cells are critical for targeting and killing tumor, virus-infected, and stressed cells as a member of the innate immune system. Individuals with post-COVID-19 conditions had an activation of NK cells [43], and the consumption of AHCC may help modulate the immune system, reducing the viral load, and leading to decreased circulating NK cell counts. In healthy human subjects, AHCC improved T-cell immune responses [15,44,45] and increased dendritic cell numbers and function [15,18]. Additional immunologic measures should be evaluated in patients with post-COVID-19 conditions treated with AHCC to better understand the pathophysiologic mechanism of disease and treatment.
Patients with COVID-19 exhibit mitochondrial dysfunction in peripheral blood mononuclear cells [46], which could lead to the inhibition of mitochondrial antiviral signaling proteins reducing the antiviral interferon response [47] and the continued symptoms of post-COVID-19 conditions. Dysfunctional mitochondria can also activate an inflammatory response as mitochondrial content is released into the cytosol [48]. While AHCC has previously been shown to have antioxidant properties and to attenuate oxidative stress [24], we specifically identified that the mitochondrial membrane potential increased after consuming AHCC for 30 days. This mitochondrial membrane potential functions as energy storage that is later used for Adenosine Triphosphate (ATP) synthesis [49,50]. Therefore, AHCC supplementation may decrease symptoms in post-COVID-19 conditions by supporting mitochondrial function and immune response.
Limitations
The small sample size was a limitation; however, the results demonstrate a strong area of interest for planning a larger-scale investigation. Second, participants had to schedule their appointments between 0700 and 1300 Monday thru Friday in order to complete the NK cell and mitochondria analysis in the afternoon. Measurements that require same-day analysis limit the number of subjects; those who have jobs may not be able to participate during those specific hours. Thus, expanding testing hours for more early morning or lunch hour time periods might be a useful strategy to reduce this limitation.
Conclusion
In this pilot study we examined the effects of AHCC® on physiological functions in patients with post-COVID-19 conditions that could lead to a larger clinical trial to investigate this supplement as a potential intervention to reduce patients’ symptom burden. The improved patient reported outcomes after consuming this mushroom supplement provide a platform for a better understanding of the clinical implications of using an over-the-counter supplement to improve the quality of life of patients who suffer from post-COVID-19 conditions.
Declarations
Conflicting interest: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding: This study was funded by the University of Kansas Medical Center, Christine A. Hartley Centennial Endowment Funds.
Ethical considerations: This study was approved by the Institutional Review Board at the University of Kansas Medical Center and exempted from registration. A written informed consent was obtained from all subjects at the beginning of the initial visit.
Acknowledgements: We acknowledge the Flow Cytometry Core Laboratory, which is sponsored, in part, by the NIH/NIGMS COBRE grant P30 GM103326 and the NIH/NCI Cancer Center grant P30 CA168524. We also acknowledge the Biomarker Core of the KU Alzheimer’s Disease Research Center related to mitochondrial analysis. We would like to thank Ms. Sally Barhydt for editing the manuscript.
References
- Department of Health and Human Services, Office of the Assistant Secretary for Health. National Research Action Plan on Long COVID. 200 Independence Ave SW, Washington, DC. 2022.
- Ballering AV, van Zon SKR, Olde Hartman TC, Rosmalen JGM, Lifelines Corona Research I. Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet. 2022; 400(10350): 452-61.
- Chen C, Haupert SR, Zimmermann L, Shi X, Fritsche LG, et al. Global Prevalence of Post-Coronavirus Disease 2019 (COVID-19) Condition or Long COVID: A Meta-Analysis and Systematic Review. J Infect Dis. 2022; 226(9): 1593-607.
- Theoharides TC. Could SARS-CoV-2 Spike Protein Be Responsible for Long-COVID Syndrome? Mol Neurobiol. 2022; 59(3): 1850-61.
- Shuwa HA, Shaw TN, Knight SB, Wemyss K, McClure FA, et al. Alterations in T and B cell function persist in convalescent COVID-19 patients. Med. 2021; 2(6): 720-35 e4.
- Afrin LB, Weinstock LB, Molderings GJ. Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome. Int J Infect Dis. 2020; 100: 327-32.
- Nunn AVW, Guy GW, Brysch W, Bell JD. Understanding Long COVID; Mitochondrial Health and Adaptation-Old Pathways, New Problems. Biomedicines. 2022; 10(12).
- Stefano GB, Ptacek R, Ptackova H, Martin A, Kream RM. Selective Neuronal Mitochondrial Targeting in SARS-CoV-2 Infection Affects Cognitive Processes to Induce ‘Brain Fog’ and Results in Behavioral Changes that Favor Viral Survival. Med Sci Monit. 2021; 27: e930886.
- Hoffmann M, Kleine-Weber H, Schroeder S, Kruger N, Herrler T, et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020; 181(2): 271-80 e8.
- Dennis A, Wamil M, Alberts J, Oben J, Cuthbertson DJ, et al. Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: a prospective, community-based study. BMJ Open. 2021; 11(3): e048391.
- Mantovani A, Morrone MC, Patrono C, Santoro MG, Schiaffino S, et al. Long Covid: where we stand and challenges ahead. Cell Death Differ. 2022; 29(10): 1891-900.
- Singh KK, Chaubey G, Chen JY, Suravajhala P. Decoding SARS-CoV-2 hijacking of host mitochondria in COVID-19 pathogenesis. Am J Physiol Cell Physiol. 2020; 319(2): C258-C67.
- Wood E, Hall KH, Tate W. Role of mitochondria, oxidative stress and the response to antioxidants in myalgic encephalomyelitis/chronic fatigue syndrome: A possible approach to SARS-CoV-2 ‘long-haulers’? Chronic Dis Transl Med. 2021; 7(1): 14-26.
- Panda SK, Luyten W. Medicinal mushrooms: Clinical perspective and challenges. Drug Discov Today. 2022; 27(2): 636-51.
- Shin MS, Park HJ, Maeda T, Nishioka H, Fujii H, et al. The Effects of AHCC(R), a Standardized Extract of Cultured Lentinura edodes Mycelia, on Natural Killer and T Cells in Health and Disease: Reviews on Human and Animal Studies. J Immunol Res. 2019; 2019: 3758576.
- Smith JA, Mathew L, Gaikwad A, Rech B, Burney MN, et al. From Bench to Bedside: Evaluation of AHCC Supplementation to Modulate the Host Immunity to Clear High-Risk Human Papillomavirus Infections. Front Oncol. 2019; 9: 173.
- Takanari J, Sato A, Waki H, Miyazaki S, Uebaba K, et al. Effects of AHCC(R) on Immune and Stress Responses in Healthy Individuals. J Evid Based Integr Med. 2018; 23: 2156587218756511.
- Chowdhury AH, Camara M, Verma C, Eremin O, Kulkarni AD, et al. Modulation of T Regulatory and Dendritic Cell Phenotypes Following Ingestion of Bifidobacterium longum, AHCC((R)) and Azithromycin in Healthy Individuals. Nutrients. 2019; 11(10).
- Dea-Ayuela MA, Segarra S, Serrano DR, Bolas-Fernandez F. Nucleotides and AHCC Enhance Th1 Responses In Vitro in Leishmania-Stimulated/Infected Murine Cells. Molecules. 2020; 25(17).
- Mallet JF, Graham E, Ritz BW, Homma K, Matar C. Active Hexose Correlated Compound (AHCC) promotes an intestinal immune response in BALB/c mice and in primary intestinal epithelial cell culture involving toll-like receptors TLR-2 and TLR-4. Eur J Nutr. 2016; 55(1): 139-46.
- Spierings EL, Fujii H, Sun B, Walshe T. A Phase I study of the safety of the nutritional supplement, active hexose correlated compound, AHCC, in healthy volunteers. J Nutr Sci Vitaminol (Tokyo). 2007; 53(6): 536-9.
- Smith JA, Gaikwad AA, Mathew L, Rech B, Faro JP, et al. AHCC(R) Supplementation to Support Immune Function to Clear Persistent Human Papillomavirus Infections. Front Oncol. 2022; 12: 881902.
- Nogusa S, Gerbino J, Ritz BW. Low-dose supplementation with active hexose correlated compound improves the immune response to acute influenza infection in C57BL/6 mice. Nutr Res. 2009; 29(2): 139-43.
- Haidari M, Zhang W, Wakame K. Disruption of endothelial adherens junction by invasive breast cancer cells is mediated by reactive oxygen species and is attenuated by AHCC. Life Sci. 2013; 93(25-26): 994-1003.
- Fries JF, Bruce B, Cella D. The promise of PROMIS: using item response theory to improve assessment of patient-reported outcomes. Clin Exp Rheumatol. 2005; 23(5 Suppl 39): S53-7.
- PROMIS (Patient Reported Outcomes Measurement Information System). Fatigue: A brief guide to the PROMIS Fatigue Instruments. 2019. https://staging.healthmeasures.net/images/PROMIS/manuals/PROMIS_Fatigue_Scoring_Manual.pdf (accessed April 28 2023).
- Webster K, Cella D, Yost K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: properties, applications, and interpretation. Health Qual Life Outcomes. 2003; 1: 79.
- Choi SW, Victorson DE, Yount S, Anton S, Cella D. Development of a conceptual framework and calibrated item banks to measure patient-reported dyspnea severity and related functional limitations. Value Health. 2011; 14(2): 291-306.
- PROMIS (Patient Reported Outcomes Measurement Information System). Cognitive Function: A brief guide to the PROMIS Cognitive Function instruments. 2019. https://staging.healthmeasures.net/images/PROMIS/manuals/PROMIS_Cognitive_Function_Scoring_Manual.pdf (accessed April 28 2023).
- Langer M. Epic PROMIS (Patient Reported Outcomes Measurement Information System) Collaborative. The Impact of COVID-19 on Patient Reported Outcomes (PRO) Administration: Relevant PRO domains and PROMIS measures. 2020.
- Ganesh R, Ghosh AK, Nyman MA, Croghan IT, Grach SL, et al. PROMIS Scales for Assessment of Persistent Post-COVID Symptoms: A Cross Sectional Study. J Prim Care Community Health. 2021; 12: 21501327211030413.
- Macchi Z, Wang Y, Moore D, Katz J, Saperstein D, et al. A multi-center screening trial of rasagiline in patients with amyotrophic lateral sclerosis: Possible mitochondrial biomarker target engagement. Amyotroph Lateral Scler Frontotemporal Degener. 2015; 16(5-6): 345-52.
- Statland JM, Moore D, Wang Y, Walsh M, Mozaffar T, et al. Rasagiline for amyotrophic lateral sclerosis: A randomized, controlled trial. Muscle Nerve. 2019; 59(2): 201-7.
- Aviles H, O’Donnell P, Orshal J, Fujii H, Sun B, et al. Active hexose correlated compound activates immune function to decrease bacterial load in a murine model of intramuscular infection. Am J Surg. 2008; 195(4): 537-45.
- Aviles H, O’Donnell P, Sun B, Sonnenfeld G. Active hexose correlated compound (AHCC) enhances resistance to infection in a mouse model of surgical wound infection. Surg Infect (Larchmt). 2006; 7(6): 527-35.
- Hashimoto D, Satoi S, Ishikawa H, Kodera Y, Kamei K, et al. Efficacy of active hexose correlated compound on survival of patients with resectable/borderline resectable pancreatic cancer: A study protocol for a double-blind randomized phase II study. Trials. 2022; 23(1): 135.
- Kamiyama T, Orimo T, Wakayama K, Kakisaka T, Shimada S, et al. Preventing Recurrence of Hepatocellular Carcinoma After Curative Hepatectomy With Active Hexose-correlated Compound Derived From Lentinula edodes Mycelia. Integr Cancer Ther. 2022; 21: 15347354211073066.
- Yanagimoto H, Satoi S, Yamamoto T, Hirooka S, Yamaki S, et al. Alleviating Effect of Active Hexose Correlated Compound (AHCC) on Chemotherapy-Related Adverse Events in Patients with Unresectable Pancreatic Ductal Adenocarcinoma. Nutr Cancer. 2016; 68(2): 234-40.
- Chauhan P, Pathak V, Kumar D, Upadhyay A, Chatterjee A, et al. Post and long-COVID conditions: Epidemiology, clinical symptoms and the prevention and treatment. Journal of Medical Evidence. 2022; 3(2): 149-54.
- Pierce JD, Shen Q, Cintron SA, Hiebert JB. Post-COVID-19 Syndrome. Nurs Res. 2022; 71(2): 164-74.
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: Major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023; 21(3): 133-46.
- Du M, Ma Y, Deng J, Liu M, Liu J. Comparison of Long COVID-19 Caused by Different SARS-CoV-2 Strains: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022; 19(23).
- Vojdani A, Koksoy S, Vojdani E, Engelman M, Benzvi C, et al. Natural Killer Cells and Cytotoxic T Cells: Complementary Partners against Microorganisms and Cancer. Microorganisms. 2024; 12(1).
- Yin Z, Fujii H, Walshe T. Effects of active hexose correlated compound on frequency of CD4+ and CD8+ T cells producing interferon-gamma and/or tumor necrosis factor-alpha in healthy adults. Hum Immunol. 2010; 71(12): 1187-90.
- Belay T, Fu CL, Woart A. Active Hexose Correlated Compound Activates Immune Function to Decrease Chlamydia trachomatis Shedding in a Murine Stress Model. J Nutr Med Diet Care. 2015; 1(1).
- Ajaz S, McPhail MJ, Singh KK, Mujib S, Trovato FM, et al. Mitochondrial metabolic manipulation by SARS-CoV-2 in peripheral blood mononuclear cells of patients with COVID-19. Am J Physiol Cell Physiol. 2021; 320(1): C57-C65.
- Shi CS, Qi HY, Boularan C, Huang NN, Abu-Asab M, et al. SARS-coronavirus open reading frame-9b suppresses innate immunity by targeting mitochondria and the MAVS/TRAF3/TRAF6 signalosome. J Immunol. 2014; 193(6): 3080-9.
- Luna-Sanchez M, Bianchi P, Quintana A. Mitochondria-Induced Immune Response as a Trigger for Neurodegeneration: A Pathogen from Within. Int J Mol Sci. 2021; 22(16).
- Zorova LD, Popkov VA, Plotnikov EY, Silachev DN, Pevzner IB, et al. Mitochondrial membrane potential. Anal Biochem. 2018; 552: 50-9.
- Bizjak DA, Ohmayer B, Buhl JL, Schneider EM, Walther P, et al. Functional and Morphological Differences of Muscle Mitochondria in Chronic Fatigue Syndrome and Post-COVID Syndrome. Int J Mol Sci. 2024; 25(3).