Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Vijayan Sharmila, MS1*; Priyanka Yoga P, MS2; Prudhvinath Reddy A, MD3; Mithilesh A, MD4
*Corresponding Author: Vijayan Sharmila
Professor and Head, Department of Obstetrics & Gynecology, All India Institute of Medical Sciences (AIIMS), Mangalagiri, Andhra Pradesh, India.
Email: sharu_jipmer@yahoo.co.in
Article Info
Received: Sep 09, 2024
Accepted: Oct 03, 2024
Published: Oct 10, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Sharmila V (2024).
Citation: Sharmila V, Yoga PP, Reddy AP, Mithilesh A. Cesarean Scar Defect, A Niche of Concern!. J Clin Med Surgery. 2024; 4(2): 1166.
Letter to editor
Isthmocele or post-caesarean niche, refers to a diverticulum at the site of a caesarean scar. Risk factors include multiple caesarean, a retroflexed uterus, labor before caesarean, low cervical incisions, and certain suturing techniques. Patients may be asymptomatic or experience post-menstrual spotting due to blood collection in the pouch or from adenomyotic deposits. This defect can also cause infertility by affecting cervical mucus, sperm quality, and embryo implantation. Rare complications include abscess formation or caesarean scar pregnancy. Differential Diagnosis for isthmocele include prominent endocervical glands, Gartner’s duct cyst and cystic adenomyosis. We report a case of Isthmocele in a multiparous women who presented with Abnormal uterine bleeding diagnosed by Magnetic Resonance Sonography (MRI).
A 27-year-old woman with a history of two previous caesarean sections presented with abnormal uterine bleeding for 4 months. Her last childbirth was five years back, and her menstrual cycles had become irregular, occurring every 20 to 25 days, accompanied by heavy menstrual bleeding. A transvaginal ultrasound revealed a normal-sized uterus and a 2.7 x 1.3 cm cystic outpouching lesion along the anterior uterine isthmus near the previous caesarean scar. Mild perilesional vascularity was noted on color Doppler. Further assessment with MRI confirmed the presence of a cystic outpouching 1.5 x 2 cm at the anterior uterine isthmus near the caesarean scar. There was no extension into the endocervical canal or the cervix (Figure 1). There was evidence of T2 hyperintense T1 hypointense lesion measuring 1 x 2 cm within endometrial cavity adjacent to the cystic outpouching without any diffuse restriction suggestive of endometrial polyp. The MRI findings were suggestive of isthmocele with adjacent endometrial polyp.
Radiological imaging is crucial for diagnosing isthmocele. Transvaginal ultrasonography is the preferred first-line imaging, typically showing a wedge-shaped defect in the lower uterine segment. The contents of the isthmocele may appear anechoic or contain internal echoes, and the width and depth of the defect can be measured. Saline-infused sonohysterogram and hysterosalpingogram can also help delineate the defect, although the latter cannot measure scar dimensions. MRI provides the most detailed confirmation, allowing for the measurement of myometrial thickness and characterization of the cyst’s contents. Simple fluid appears dark on T1 fat-suppressed images and bright on T2, while hemorrhagic content shows as bright on T1 and variable on T2, sometimes with rim enhancement. Focal abscess formation shows iso-to-bright on T1 and bright on T2, with thick rim enhancement post-contrast.
Management of symptomatic cases may include conservative treatment with oral contraceptives. If unsuccessful, hysteroscopic or laparoscopic correction can be performed to drain the accumulated menstrual blood. Around 80% of patients experience full relief of symptoms after surgery.
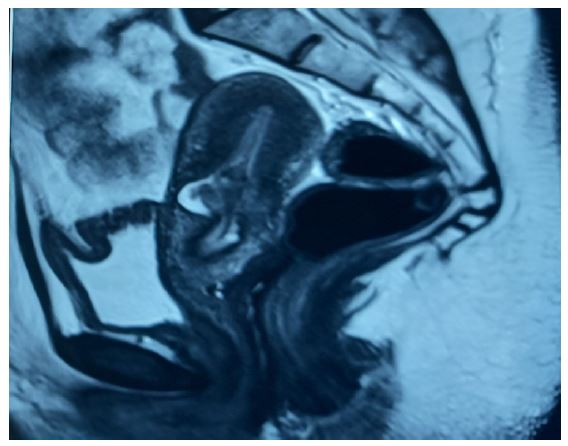
Figure 1: MRI image showing cystic outpouching lesion along the anterior uterine isthmus near the previous caesarean scar suggestive of isthmocele.
References
- Allornuvor G, Xue M, Zhu X, Xu D. The definition, aetiology, presentation, diagnosis, and management of previous cesarean scar defects. J Obstetrics and Gynecology. 2013; 33: 759‐63.
- Tower AM, Frishman GN. Cesarean scar defects: An unrecognized cause of abnormal uterine bleeding and other gynecologic complications. J Minim Invasive Gynecol. 2014; 20: 562-572.
- Raimondo G, Grifone G, Raimondo D, Seracchioli R, Scambia G, et al. Hysteroscopic treatment of symptomatic cesarean induced isthmocele: A prospective study. J Minim Invasive Gynecol. 2015; 22(2): 297-301.