Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 4
Open Access
Volume 4
Andrea Lechiancole1*; Enrico Spagna1; Sandro Sponga1,2; Andriy Dralov1; Arianna Semeraro1; Stefano Copetti1; Cesare Puricelli1†; Uberto Bortolotti1; Ugolino Livi1; Igor Vendramin1,2
*Corresponding Author: Andrea Lechiancole
Department of Medicine (DMED), University Hospital of Udine, P.le S.M. Della Misericordia 15, Udine, Italy.
Tel: 39-432-552430, Fax: 39-432-552975;
Email: andrea.lechiancole@asufc.sanita.fvg.it
Article Info
Received: Aug 21, 2024
Accepted: Sep 10, 2024
Published: Sep 17, 2024
Archived: www.jclinmedsurgery.com
Copyright: © Lechiancole A (2024).
Abstract...
Median sternotomy still represents the most widely used approach in cardiac surgery. Closure of the sternotomy incision is generally performed using stainless steel wires, a procedure which, however, is not completely free of complications. These are mainly represented by sternal fracture, sternal dehiscence and infections which may significantly increase surgical morbidity and mortality. We present here a new device, the Sternette® system, designed to facilitate sternal closure and prevent postoperative sternotomy wound complications. The peculiar configuration of this device minimize the risk of cutting the sternal bone which may be increased postoperatively, especially in subject with fragile sternum, during the breathing movements of the chest wall. We have used this device in a series of 31 patients in whom it proved effective and free of any early and late postoperative complications.
Keywords: Median sternotomy; Sternal closure; Sternal dehiscence; Sternal closure device.
Citation: Lechiancole A, Spagna E, Sponga S, Dralov A, Copetti S, et al. Sternette®: An Alternative Closure Device after Median Sternotomy. J Clin Med Surgery. 2024; 4(2): 1164.
Introduction
Since its introduction more than one century ago [1], longitudinal Median Sternotomy (MS) is still considered today the standard approach used by most surgeons to treat all congenital and acquired heart diseases [2]. Indeed, MS not only provides adequate exposure of all intrapericardial cardiac structures and great vessels, but it also may be used in thoracic surgery for mediastinal tumor resection and to address certain pathologies of the lungs, stem bronchi and inferior trachea [2].
Traditionally, MS is closed by re-approximating the two sternal halves with 6 to 8, either interrupted or figure-of-eight, stainless steel wires, passed through the bone thickness or the intercostal spaces [3]; however, metallic wires may rupture or cut through the bone especially in case of evident sternal fragility or osteoporosis or unequal sternal sawing. Such complications, reported in up to 6% of patients, may be facilitated by vigorous chest wall movements as such during postoperative respiratory physiotherapy or by prolonged mechanical ventilation [4-7].
Although employment of wires even today remains the most used method of sternal closure several alternative techniques have been proposed, including various types of clips or plates made of different metals or cables and bands [8-14]. In this paper we aimed to present an innovative device for sternal closure, the Sternette® system, devised by one of the authors (CP), and registered in the “Ufficio Italiano Brevetti e Marchi” of the Italian Ministry of Business and Made in Italy, with protocol number 1043292, which could facilitate sternal closure and reduce the complications associated to the use of traditional methods.
Material and methods
Device characteristics
Sternette® consists of a screw-adjusted double-branched clip which is placed at the level of manubrium and parasternally in the intercostal spaces hooking the sternal halves (Figure 1A). By using an adjustable screwdriver the 2 branches of the device are tightened allowing progressive approximation of the sternal edges (Figure 1B,C). Sternette® is designed to have clips applied separately into the sternum with a device fixer. There are 4 available sizes of the device according to the width of the sternum: 7.5 mm, 9.0 mm, 12.0 mm, 15.0 mm, while the length of the notched arms is 9 mm.
Device positioning
At the end of the surgical procedure and after hemostasis is achieved the 2 sternal halves are manually approximated. At this point, 1 to 2 holes are created at the level of the manubrium by a punch-cutter device, and 3 to 4 parasternal intercostal spaces on each side are freed from pre-sternal muscular tissue in order to evidence the costal attachments. The width of the sternum is then measured by a sizer and Sternette® clips of adequate size are positioned so that both arms surround the corresponding portion of the sternum. Clips are then inserted into the screwing system, which joins the sternal halves together by their progressive approximation (Figure 2). After implant the clips are easily recognizable on standard chest x-ray (Figure 3).
In cases of emergency re-exploration or redo-sternotomy, the clip can be cut with a heavy wire cutter in the thin horizontal component, near the screw.
Study population
Sternal closure using Sternette® clips was prospectively performed in a series of 31 patients at our Institution from 2006 to 2011 (Institutional Ethics Committee approval number 37416). There were 25 males (81%) and 6 females (19%) with a mean age of 71±5 years. Specific risk factors were hypertension in 28 of them (90%), dyslipidemia in 27(87%), type-2 diabetes mellitus in 13(42%) and chronic obstructive pulmonary disease in 11(32%). Table 1 summarizes the preoperative clinical characteristics of this series.
Most patients had undergone Coronary Artery Bypass Grafting (CABG) (n=29, 91%) using a single internal mammary artery and vein grafts, while in in 3 cases the device was employed for sternal closure in patients that required sternal reconstruction after deep sternal wound infection treatment (Table 2).
Statistical analysis
Continuous variables were expressed as mean ± standard deviation or median and interquartile range, and data analyzed using the Shapiro-Wilk test to verify the normal distribution. Categorical variables were presented as absolute numbers and percentages. Analyses were performed using the Statistical Package for Social Sciences (SPSS) program (Chicago, IL, USA).
Results
There was one operative death (3%) after CABG due to multiorgan failure; death was not associated with sternal dehiscence or infection. In all patients adequate sternal closure was obtained. Postoperatively no major complications were observed as well as no procedure-related adverse events. In one patient a superficial wound infection, not involving the sternum, occurred which was treated successfully with antibiotic therapy and local medications.
During a mean follow-up period of 7±4 years, there were 4 late deaths. No complications related to Sternette® implant, such as fracture and skin erosion or infection, were reported.
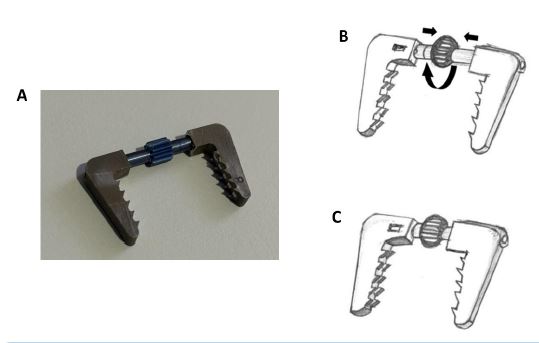
Figure 1: (A) The Sternette® synthesis device. Assembling the components, turning the wheel allows for vary the length to adapt to the sternal size. (B) open and (C) tightened configurations.
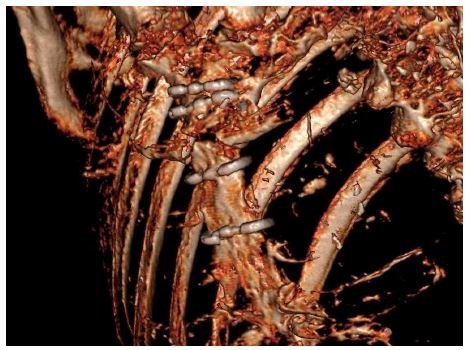
Figure 2: 3D CT scan reconstruction of healed sternum with Sternette® device.

Figure 3: Appearance of the device in lateral (A) and anteroposterior (B) chest x-ray.
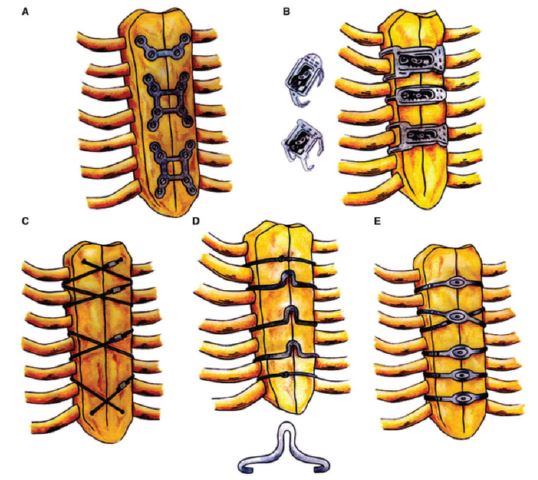
Figure 4: Various methods of sternotomy closure using rigid plate fixation (A), talon (B), titanium cables (C), nitinole clips (D) and flat wires (E). (Reproduced with permission from Ref #19).
Table 1: Preoperative patient characteristics.
| No. of patients | 31 |
|---|---|
| Males n. (%) | 25(81) |
| Mean age, years ± SD | 71±5 |
| Arterial hypertension, n. (%) | 28 (90) |
| Dyslipidemia, n (%) | 27(87) |
| Type 2 diabetes, n. (%) | 13(42) |
| COPD, n. (%) | 11(32) |
| KDIGO >3, n. (%) | 3(1) |
| Mean BMI ± SD | 31±6 |
SD: Standard Deviation; COPD: Chronic Obstructive Pulmonary Disease; KDIGO: Kidney Disease Improving Global Outcomes; BMI: Body Mass Index.
Table 2: Surgical data and post-implant complications.
| No. of patients | 31 |
|---|---|
| Indication | |
| Post-CABG, n. (%) | 29(91) |
| Sternal closure after DSWI | 3(9) |
| Results | |
| 30 - day mortality, n (%) | 1(3) |
| Post-implant device malfunction, n. (%) | - |
| Post-implant sternal dehiscence, n. (%) | - |
CABG: Coronary Artery Bypass Grafting; DSWI: Deep Sternal.
Table 3: Summary of reported experiences with various sternal closure devices.
| Author | Device | N. of pts | Post-op complications | Follow-up |
|---|---|---|---|---|
| Levin et al. 2010 [8] | Sternal Talon® ® (KLS Martin Group, Jacksonville, FL) | 42 | No DSWI | NA |
| Nikolaidis et al. 2012 [9] | Nitinol clips (Praesidia, Bologna, Italy) | 235 | DSWI in 4 patients (1.7%) | NA |
| Boustany et al. 2014 [10] | FlatWire Sternal Closure System (Penn United Tech. Inc., Cabot, PA) | 63 | No post-op complicatiuons | 1 year |
| Dunne et al. 2016 [11] | Pioneer Cable System (Pio- neer Surgical Technology, Inc., Marquette, MI) | 135 | DSWI in 5 patients (3.7%) | 4 weeks |
| Allen et al. 2017 [12] | SternaLock® Blu (Zimmer Biomet, Jacksonville, FL) | 116 | No DSWI | 6 months |
| Nezafati et al. 2019 [14] | ZipFixTM (Synthes GmbH, Oberdorf, Switzerland) | 168 | Superficial infection in 2 patients (1.2%) | 1 year |
DSWI: Deep Sternal Wound Infection; NA: Not Available.
Discussion
MS was first proposed by Milton in 1897 to excise massive tuberculous lymph nodes compressing the mediastinum, but it was reintroduced, ‘as Milton procedure’ only in 1957 by Julian and associates as surgical approach in open heart operations [15]. Despite the increasing use of minimally invasive techniques, MS is still considered as the gold-standard procedure in cardiac surgery to access the heart and mediastinal great vessels. Closure of the sternotomy incision has been obtained initially with multiple, heavy polyester sutures which have been recognized to be associated to increased incidence of wound infections, wound-related pain and late wound complications [16]. Therefore, sternal closure with wires has become the standard method because of the ease and speed of use, the relatively low complication rate, and the low cost of wires [5].
MS, together with eventual sternal closure, are generally quite standard procedures; nevertheless, both are important surgical steps which, if not properly and correctly per-formed, may affect short- and long-term morbidity and mortality [2]. Indeed, once the sternum is divided, it must be adequately stabilized at the end of any procedure. In fact, incorrect sternal closure may lead to various complications ranging from sternal instability, with pain and dismal consequences on respiration, to sternal dehiscence, superficial infections of the sternotomy wound and, more importantly, to mediastinitis, an often catastrophic event [3,4].
The sternotomy incision is closed passing single stainless steel wires through or around the sternal bone; the wire ends are then progressively twisted together to approximate the sternal halves and close the incision. Several varieties of this procedure have been proposed to minimize tearing of the sternal bone by better distributing the forces acting upon the sternal hedges, such as the figure-of-eight suture or the Robicsek techniques and its modifications [14].
Closure of the median sternotomy is apparently a straightforward procedure which, however, represents an important step of any cardiac operations. In fact, inappropriate sternal closure may predispose to sternal dehiscence, infection and mediastinitis causing increased pain at the incision site, difficulty in coughing and breathing, and therefore pro-longed hospitalization, increased treatment costs, and most importantly, increased morbidity and mortality. Risk factors for sternal dehiscence include age at operation, female sex, osteopenia, malnutrition, bilateral internal thoracic artery harvesting, diabetes mellitus, and postoperative infection [18].
To minimize such events, in recent years, new devices have been introduced clinically such as clips, bands or plates to be used, which have been shown to be particularly effective during complex sternal repairs [19] (Figure 4). Among these, nitinol clips, in a computational model, have shown extreme elasticity with shape memory which should allow multiple staples placed along the sternum to promote fast and safe recovery by maintaining constant clamping pressure at the sternotomy midline [20]. However, none of these are free from complications and have demonstrated significant benefits over the standard techniques in patients with risk factors for sternal wound dehiscence [14]. In particular, most of these devices have not evidenced superior advantages in pain or analgesic re-quirements relative to standard wire closure after median sternotomy [14]. Another limitation of most of the reports on the clinical application of such devices is represented by the short-term follow-up data which, when available, do not exceed the first postoperative year in most of them [10,14]. Therefore, it is not possible to verify in the long term the stability of the repair and incidence of possible late complications, such as fracture or dislodgement, inflammatory reaction or tissue necrosis in skinny patients, as well as the occurrence of reinfection when sternal closure was performed after successful treatment of mediastinitis.
We have employed in a small series of patients a new device, the Sternette® system, and summarized here the preliminary results. This device has proved to be simple and intuitive to use and, owing to the adjustable screw-system for clip tightening, it provides an elastic support to the movements of both sternum and chest wall during respiration. This feature, combined with the smooth and larger surfaces of the clip branches exerting a low-er pressure on the sternal surface, could help reducing the risk of sternal rupture. Furthermore, the clips are positioned on the anterior surface of the sternum and this should avoid the risk of intrapericardial bleeding which may occur by inadvertent injury to the inter-costal vessels by the wires.
This device has proved to be particularly advantageous during sternal closure after recovery from a deep sternal wound infection or mediastinitis. In fact, there is no need for extended dissection of the sub-sternal planes to mobilize the sternal halves for wire closure with the risk of injury to mediastinal structures with potentially severe bleeding com-plications; as shown in 3 of our patients, minimal dissection of the pre-sternal tissues was sufficient to implant the Sternette® to treat a post-infection sternal dehiscence. Moreover, although the clip does not encircle the sternum, no posterior displacement of sternal edged was observed, probably because the accurate and homogeneous tension exerted on the sternum, and the length and indentation of the clip arms.
On the contrary, in patients with a very thin sternum, it may be useful to avoid insert-ing the clip into the caudal portion of the sternum, to prevent the clip arm from being too deep into the chest, causing injury to the right ventricle or atrium.
In our preliminary series of cases, this device has proven to be safe and effective, with satisfactory results, that are not inferior compared to the traditional closure with steel wires in terms of sternal stability. Moreover, we believe that Sternette® clips could be particularly useful and effective in patients at high-risk for sternal dehiscence.
Larger comparative studies are needed to demonstrate advantages of the Sternette® device over other sternal closure systems.
Conclusion
The Sternette® system represents an innovative device, designed to prevent complications related to sternal closure with steel wires. In the present experience, its use has proven to be safe, free of complications and to provide sternal stability over time. Although further studies on larger patient populations are required, the Sternette® system appears a re-liable tool with definite advantages in patients who require sternal closure after previous dehiscence or infection.
Declarations
Author contributions: Conceptualization, C.P. and U.L.; methodology, E.S.; formal analysis, A.L.; investigation, A.L., U.B.; data curation, E.S., A.S., S.C.; writing-original draft preparation, A.L.; writing-review and editing, U.B.; visualization, all authors.; supervision, I.V., S.S and U.L. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional review board statement: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Azienda Sanitaria Universitaria Friuli Centrale (protocol code 62724, approved in 16 th december 2005).
Informed consent statement: Informed consent was obtained from all subjects involved in the study.
Data availability statement: The data presented in this study are available on request from the corresponding author.
Conflicts of interest: The authors declare no conflicts of interest.
References
- Julian OC, Lopez-Belio M, Dye WS, Javid H, Grove WJ. The median sternal incision in intracardiac surgery with extracorporeal circulation: a general evaluation of its use in heart surgery. Surgery. 1957; 42:753-61.
- Reser D, Caliskan E, Tolboom H, Guidotti A, Maisano F. Median sternotomy. Multimed Man Cardiothorac Surg. 2015; 2015: mmv017. doi: 10.1093/mmcts/mmv017.
- Çiçek S. Sternal closure: Wires are still the king! J Thorac Cardiovasc Surg. 2018; 156: 1596-1597. doi: 10.1016/j.jtcvs.2018.04.106.
- Aykut K, Albayrak G, Kavala A, Guzelogu M, Karaarslan K, et al. Early repair of sternal instability prevents mediastinitis. World J Cardiovasc Surg. 2014; 4: 13-16 doi.org/10.4236/wjcs.2014.42003
- Abu-Omar Y, Kocher GJ, Bosco P, Barbero C, Waller D, et al. European Association for Cardio-Thoracic Sur-gery expert consensus statement on the prevention and management of mediastinitis, Eur J Cardio-Thoracic Surg. 2017; 51: 10-29, https://doi.org/10.1093/ejcts/ezw326.
- Hota P, Dass C, Erkmen C, Donuru A, Kumaran M. Poststernotomy complications: A multimodal review of normal and abnormal postoperative imaging findings. Am J Roentgenol 2018; 211: 1194-1205. doi.org/10.2214/AJR.18.19787.
- Scott NM, Lotto RR, Spencer E, Grant MJ, Penson P, et al. Risk factors for post sternotomy wound complications across the patient journey: A systematised review of the literature. Heart & Lung. 2022; 55: 89-101. https://doi.org/10.1016/j.hrtlng.2022.04.013.
- Levin LS, Miller AS, Gajjar AH, Bremer KD, Spann J, et al. An innovative approach for sternal closure. Ann Thorac Surg. 2010; 89: 1995-1999. doi: 10.1016/j.athoracsur.2010.01.089.
- Nikolaidis N, Karangelis D, Mattam K, Tsang G, Ohri S. The use of Nitinol clips for primary sternal closure in cardiac surgery. Ann Thorac Cardiovasc Surg. 2013; 19: 330-334. doi: 10.5761/atcs.nm.12.01947.
- Boustany AN, Ghareeb P, Lee K. Prospective, randomized, single blinded pilot study of a new FlatWire based sternal closure system. J Cardiothorac Surg. 2014; 9: 97. doi: 10.1186/1749-8090-9-97.
- Dunne B, Murphy M, Skiba R, Wang X, Ho K, et al. Sternal cables are not superior to traditional sternal wiring for preventing deep sternal wound infection. Interact Cardiovasc Thorac Surg. 2016; 22(5): 594-8. doi: 10.1093/icvts/ivw017.
- Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, et al. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017; 153: 888-896.e1. doi:10.1016/j.jtcvs.2016.10.093.
- Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, et al. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018; 156: 1589-1595.e1. doi: 10.1016/j.jtcvs.2018.04.025.
- Nezafati P, Shomali A, Kahrom M, Omidvar Tehrani S, Dianatkhah M, et al. ZipFix Versus Conventional Sternal Clo-sure: One-Year Follow-Up. Heart Lung Circ. 2019; 28: 443-449. doi: 10.1016/j.hlc.2018.01.010.
- Dalton ML, Connally SR, Sealy WC. Julian’s reintroduction of Milton’s operation. Ann Thorac Surg. 1992; 53: 532-533. doi: 10.1016/0003-4975(92)90293-d.
- Malhotra A, Garg P, Bishnoi AK, Pendro V, Sharma P, et al. Is steel wire closure of sternotomy better than polyester suture closure? Asian Cardiovasc Thorac Ann. 2014; 22: 409-415. doi: 10.1177/0218492313489696.
- Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018; 156: 178-186. doi: 10.1016/j.jtcvs.2018.02.033.
- Song Y, Chu W, Sun J, Liu X, Zhu H, et al. Review on risk factors, classification, and treatment of sternal wound infec-tion. J Cardiothorac Surg. 2023; 18: 184. https://doi.org/10.1186/s13019-023-02228-y.
- Cataneo DC, Dos Reis TA, Felisberto G, Rodrigues OR, Cataneo AJM. New sternal closure methods versus the standard clo-sure method: systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2019; 28: 432-440. doi:10.1093/icvts/ivy281.
- Subasi O, Torabnia S, Lazoglu I. In silico analysis of superelastic Nitinol staples for trans-sternal closure. J Mech Behav Biomed Mater. 2020; 107: 103770. doi.org/10.1016/j.jmbbm.2020.103770.