Introduction
Pneumatosis intestinalis is the presence of gas-filled cysts
in submucosa or subserosa of small or large bowel wall and is
divided into two categories: life-threatening pneumatosis intestinalis and benign pneumatosis intestinalis. Distinguishing between pneumatosis cystoides intestinalis and life-threatening
pneumatosis intestinalis may be challenging, although computed tomography scan allows the detection of additional findings
that may suggest an underlying, potentially cause of pneumatosis intestinalis. To correctly manage the patients affected by this
disease is important to differentiate the two types of pneumatosis and investigate the correct pathogenesis that nowadays is
still unclear altought some causes have been theorized.
According to literature, approximately 85% of cases are
thought to be secondary to coexisting mechanical or bacterial disorders of the gastrointestinal tract or the respiratory system [1].
The mechanical theory, which is the most accepted explanation, suggests that gas under pressure is forced into the bowel
wall through a mucosal defect associated with trauma, surgery,
endoscopy and bowel obstruction.
Second, there is the bacterial theory. In animal experiments,
introduction of bacteria into the bowel wall by injection has
been shown to cause PCI. The pulmonary theory has been criticized as the assumption that gas travels from ruptured alveoli
through the mediastinum into retroperitoneal space and finds
its way along perivascular spaces through the mesentery into
the bowel wall could not be proven convincingly [2].
The presenting clinical findings may be very heterogeneous
and symptoms of pneumatosis cystoides intestinalis, depending
on the location of the gas filled cysts, may include diarrhea, constipation, rectal bleeding, mucorrhoea, abdominal discomfort,
abdominal pain, urgency, malabsorption, weight loss and excessive flatus. Depending on the location of the gas filled cysts
the range of symptoms in each patient may vary enormously
[3]. Intestinal pneumatosis may lead to various complications.
The patients with pneumatosis cystoides intestinalis are usually
treated conservatively; the surgical treatment is reserved for
complications [4].
n this case report we evaluate the safety and the risk when
a conservative approach is applied in patients with PCI in accordance to the guidelines mentioned in “International Committee
of Medical Journal Editors” [5].
Case presentation
The case we are describing it is about a 81-year-old woman
with abdominal pain, nausea, vomiting, abdominal distention
and discomfort for 4 days. She did not develop fevers.
Her blood chemistry tests showed no alterations in the inflammation indices, but only a slight increase in LDH and lactates.
She was admitted from our emergency room to our radiology department for further evaluation of her symptom.
The medical history of the patient revealed arterial hypertension, mitral valve replacement for stenosis with mechanical
valve, atrial fibrillation, a PM, chronic renal failure, hypothyroidism; the patient did not report a history of gastrointestinal desease. The abdomen CT showed small share of air in the peripheral intrahepatic portal system, with arboriform appearance
(Figure 1).
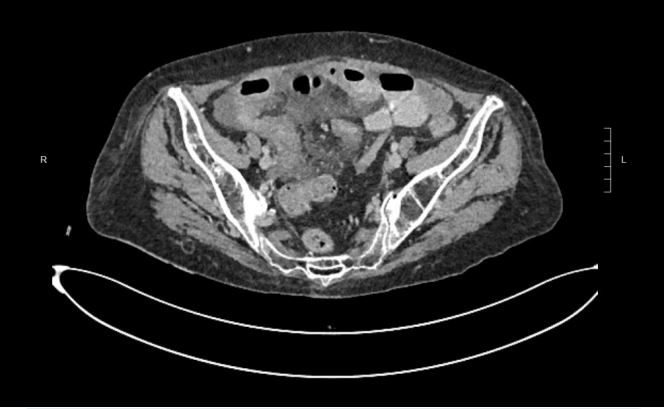
Slight fluid distension of ileal loops located in the meso-hypogastric, some of which with thickened walls with mucosal hyperemia and others with probable wall pneumatosis and associated air in the context of some respective mesenteric vascular
structures” (Figure 2).
The above-described findings were first of all due to acute
intestinal distress.
Upon admission to the hospital, the patient’s abdomen was
treatable and her abdominal pain had subsided. The biochemical parameters did not show substantial variations compared
to those performed in the emergency room, so it was decided
to postpone an emergency video laparoscopy and to continue
the clinical observation. She was managed with bowel rest, nasogastric tube decompression, hydration and broad-spectrum
antibiotics.
The day after, the biochemical parameters improved and the abdomen CT with contrast agent reported the following “no
longer appreciable the share of air in the peripheral intrahepatic portal system. Slight and fluid distension of the ileal loops is
confirmed with probable reduced wall pneumatosis compared
to the control” (Figure 3).
The finding of pneumatosis intestinalis resolved over the ensuing 3 days.
Her diet was slowly advanced after 4 days of fasting and she
was discharged home in stable condition without further surgical intervention or recurrence of the pneumatosis.
Discussion
Pneumatosis intestinalis was defined by Lerner and Gazin in
1946 as the presence of gas in an abnormal site of the body [6].
PCI is a rare condition characterized by multilocular gas-filled
cysts localized in the submucosa and subserosa of the gastrointestinal tract. The data present in the literature do not currently
allow us to ascertain the real incidence. Symptoms, if any, are
abdominal pain, diarrhea, constipation, rectal bleeding, tenesmus or weight loss and severe complications, including volvulus, intestinal obstruction, tension pneumoperitoneum, bleeding, intussusception, and intestinal perforation, may be seen.
Pneumoperitoneum and pneumoretroperitoneum can be rare
complications due to rupture of the cysts. In our case, free intraperitoneal air was secondary to a mechanical cause maybe
because of an intestinal occlusion by an intestinal volvulus subsequently resolved spontaneously
Radiological tools as plain radiographs, ultrasonography,
barium series, MDCT, MDCT colonoscopy and MRI are important for diagnosing PCI. In particular x-ray is of great importance
because it is readily available in every emergency room but only
MDCT give us higher quality and accuracy because of the advancement of multidetector technology. Cysts usually appear as
radiolucent shadows, similar to a bunch of grapes, close to the
intestinal lumen on radiographs on the contrary MDCT show
spatial resolution and is the most useful modality for diagnosing PCI and other intra-abdominal pathologies. To confirm a PCI
diagnosis is useful surgical exploration if the physical examination and imaging findings are suspicious [6].
Conclusion
The clinical condition of the patient, not only the finding of
pneumatosis intestinalis, should drive management in these
cases [3,7].
In conclusion, as we illustrated by this case report, the correct diagnosis and management of PCI is based on the results
of clinical assessment and imaging techniques. PCI also should
be kept in mind as a rare cause of pneumoperitoneum. Concordantly, it is very important for the radiologist to recognize
the abnormal findings on the MDCT or MRI studies for differentiating between medical and surgical causes of PCI. Conservative approaches, including nasogastric decompression, intestinal rest, antibiotic therapy and oxygen are recommended for
patients with positive examination findings and normal biochemical parameters who are confirmed radiologically to have
no intestinal ischemia or perforation. An urgent laparotomy is
necessary in cases of intestinal ischemia, obstruction, intestinal bleeding, or peritonitis related to high mortality rate due to
pneumatosis cystoides intestinalis. As a result, many authorities advocate an aggressive surgical approach in those patients
so definitive surgery should be performed during laparotomy
if necrosis, perforation or marked ischemia is observed in the
intestine, but no in our patient [2].
In this case report we show the opportunity of the “no treatment”. The procedure is feasible and the choice of the strategy
to be employed should be individualized based on diagnosis,
patient characteristics, availability of resources and experience
of surgical team.
Declarations
Consent for publication: Written informed consent was obtained from the patient for publication of this case report.
Ethics approval and consent to participate: Ethical approval
was not applicable.
Conflict of interest: The authors declare that they have no
conflict of interest.
Financial disclosure: The authors declared that this study
has received no financial support.
Authors’ contributions: Bonventre Giulia provided the preparation of manuscript, the conceptualization and planning of
the case report. D’Avolio Michele contributed to the diagnosis and management of the case. Mingoia Giovanni, Dominici
Domenico Marco, Nicosia Giuseppe , Sferrazza Sonia , Raspanti
Cristina , Ferrara Gabriella , Palma Antonio , Maltese Stefania
contributed to the data collection. Di Gregorio Riccardo contributed to the figures selection. Every authors read and approved
the final manuscript.
Acknowledgments: Not applicable.
References
- Micklefield GH, Kuntz HD, May B. Pneumatosis cystoides intestinalis: Case reports and review of the literature. Mater Med Pol.
1990; 22(2): 70-2. PMID: 2102980.
- Saber A. Pneumatosis intestinalis with complete remission: A
case report. Cases J. 2009; 2: 7079. doi: 10.1186/1757-1626-
0002-0000007079.
- Tchabo NE, Grobmyer SR, Jarnagin WR, Chi DS. Conservative
management of pneumatosis intestinalis. Gynecol Oncol. 2005;
99(3): 782-4. doi: 10.1016/j.ygyno.2005.08.008.
- Di Pietropaolo M, Trinci M, Giangregorio C, Galluzzo M, Miele
V. Pneumatosis cystoides intestinalis: case report and review of
literature. Clin J Gastroenterol. 2020; 13(1): 31-36. doi: 10.1007/
s12328-019-00999-3.
- International Committee of Medical Journal Editors (ICMJE). International Committee of Medical Journal Editors (ICMJE): Uniform Requirements for Manuscripts Submitted to Biomedical
Journals: Writing and editing for biomedical publication. Haematologica. 2004; 89(3): 264.
- Ogul H, Pirimoglu B, Kisaoglu A, Karaca L, Havan N, et al. Pneumatosis cystoides intestinalis: an unusual cause of intestinal
ischemia and pneumoperitoneum. Int Surg. 2015; 100(2): 221-
4. doi: 10.9738/INTSURG-D-13-00238.1.
- Brighi M, Vaccari S, Lauro A, D’Andrea V, Pagano N, et al. Cystamatic Review: Is Surgery Mandatory for Pneumatosis Cystoides
Intestinalis? Dig Dis Sci. 2019; 64(10): 2769-2775. doi: 10.1007/
s10620-019-05767-4.