Introduction
Spinal deformities refer to deformities where the curvature
of the spine is convex in the coronal plane, convex in the posterior plane, and convex in the sagittal plane. When the Cobb
angle of the deformity is greater than 90°, it is called a severe
deformity [1]. Severe spinal deformities are often accompanied
by reduced thoracic volume, pulmonary parenchymal compression, restricted diaphragm activity, airway changes, obstructed
lung ventilation, and decreased lung capacity, which in turn affect the patient’s respiratory function [2]. A survey shows that
the incidence of respiratory dysfunction in patients with severe
spinal deformities is as high as 80%, which is the main cause of
adverse events such as circulatory disorders, pulmonary hypertension, pulmonary heart disease, and even death [3]. There
is still controversy in clinical practice regarding the treatment
measures for patients with severe spinal deformities and respiratory dysfunction. In order to reduce the risk of surgical complications, most scholars advocate avoiding primary surgery
and using adjuvant treatments such as traction to reduce spinal
stiffness [4]. Currently, traction methods such as Halo Femoral
Traction (HFT) and Halo Gravity Traction (HGT) are commonly
used in clinical practice. HFT can provide strong traction and
quickly improve spinal deformities in a short period of time, but
this method greatly restricts patient activity, is not conducive
to exercising cardiovascular function, and is prone to complications such as pressure injury and pneumoconiosis. It is only
used for short-term preoperative traction [5]. HGT is a safe and
effective traction method, but it provides less corrective force
and has drawbacks such as low treatment efficiency and long
treatment cycle [6]. Halo Pelvic Traction (HPT) has been used for
the treatment of scoliosis patients since the 1970s. This method can provide strong traction around the clock and effectively
correct various spinal deformities [7]. However, traditional HPT
requires a full body traction frame, which affects patient comfort and sleep quality, limiting its clinical application [8]. In view
of this, this study improved the HPT method and applied it to
patients with severe spinal deformities and respiratory dysfunction to observe its safety and effectiveness, aiming to provide
reference for the treatment of severe spinal deformities. The
following report is presented.
Materials and methods
General information
Using a pre- and post experimental control design method,
120 patients with severe spinal deformities and respiratory
dysfunction admitted to Beijing Dawang Road Emergency Rescue Hospital from January 2019 to January 2022 were selected
as the study subjects. Inclusion criteria: ①No gender or age
limit; ②Spinal X-ray shows a Cobb angle greater than 90° for
main curvature and a Cobb angle greater than 125° for lateral
curvature; ③Accompanied by respiratory dysfunction (partial
pressure of carbon dioxide PaCO2
≥50 mmHg, forced lung capacity FVC% < 60%); ④Choose the first stage of HPT treatment
and the second stage of simple posterior column osteotomy
correction+pedicle screw internal fixation surgery; ⑤The patient voluntarily accepts this treatment plan and signs an informed consent form.
Exclusion criteria: ①Previous spinal surgery, including internal growth rod insertion, anterior release, revision surgery, etc.; ②There are contraindications for traction, such as spinal
fractures, dislocations, etc.; ③Concomitant ankylosing spondylitis, spinal tumors, spinal tuberculosis, and other spinal diseases; ④There is skin damage at the puncture point, making
it impossible to install the pelvic ring; ⑤Concomitant mental
illness, unable to cooperate with HPT treatment.
Exit criteria: ①Those who voluntarily give up during HPT
treatment; ②Severe complications such as pneumothorax,
severe atelectasis, cranial nerve injury, and lower limb paralysis may occur during the treatment process. This study was
approved by the Medical Ethics Committee of Beijing Dawang
Road Emergency Rescue Hospital.
Improvement of HPT device characteristics
The application of traditional HPT in severe spinal deformities is relatively limited, mainly due to the following reasons:
①The traction frame is distributed around the trunk and fixed
in position, which affects the patient’s supine sleep posture
and leads to poor patient tolerance [9]. ②The pelvic ring is a
closed loop, which is inconvenient to wear due to significant differences in patient body size [10]. This study improves the traditional HPT traction device by using a pelvic ring as a half ring,
which can be worn from the side, reducing the inconvenience
caused by the closed-loop structure being worn from the foot;
And place the traction rod on the front outer side of the patient,
allowing them to sleep, dress, and move on their own while still
achieving 24-hour uninterrupted traction.
Improve the installation and traction strategy of the HPT
device
The HPT device consists of a head ring, pelvic ring, and a
telescopic link. The number of screws inserted into the pelvis
depends on the patient’s bone condition and anatomical variation. All patients completed the installation of HPT devices under local anesthesia in a sterile operating room. The patient is
placed in a supine position, and the standing position is confirmed to mark the insertion point. The skin near the insertion
point is disinfected and covered with a cloth. Three 4.5 mm
or 5.5 mm diameter iliac screws are prepared to be inserted
into the top platform area between the bilateral anterior superior iliac spine and the posterior superior iliac spine. The
depth is approximately 7 cm according to the patient’s iliac
bone condition. Then place the head ring traction device and
try to maintain a consistent distance between the surrounding
gaps, with the traction rod placed on the front outer side of
the patient. The traction frame was constructed within 3-5 days
to facilitate the patient’s full adaptation to the head ring and
pelvic screws. After the framework construction is completed,
traction treatment begins. In the first week, the spiral traction
frame is extended at a speed of 0.5 cm/d. Starting from the second week, adjust to 0.3-0.5 cm/d and intermittently adjust the
traction frame to avoid pain intolerance and nerve complications caused by repeated traction. Check the patient’s cranial
and limb nerves daily. Once neurological complications occur,
such as numbness, weakness, tongue deviation, and difficulty
swallowing, the traction should be stopped immediately, and
the traction rod should be appropriately shortened. If necessary, the length before traction should be shortened, and symptomatic treatment should be combined. After the symptoms
disappear, traction should be given. Perform daily nail care to keep the skin near the nail path clean and dry, and avoid longterm retention that may cause local infections. Regularly check
if the screws are loose or displaced. If the patient experiences
pain around the nail path, it often indicates that the screws are
loose and should be tightened in a timely manner. Review X-ray
films every 3 weeks during the traction period.
Surgical plan
After the first stage of traction treatment, a posterior spinal scoliosis correction surgery was performed under selective
general anesthesia, and HPT traction was maintained during
the operation. The patient is placed in a prone position, and
the screw at the head of the traction rod is loosened 3-5 cm
upwards to fully expand and further correct spinal deformities
during surgery. Post operative support protection for 3 months,
release the support immobilization according to the bone fusion situation, and adhere to rehabilitation exercise. Follow up
with full length spinal X-ray at 3 months, 6 months, 12 months,
and every 6 months thereafter
Observation indicators
Imaging indicators: The imaging examinations were performed on a standing position X-ray of the entire length of the
spine, with a follow-up every 3 weeks during traction. Collect
data on the coronal and sagittal planes of the entire spine in
the standard standing position before HPT traction, during the
last traction follow-up, after internal fixation surgery (the first
month after internal fixation surgery), and during the last follow-up.
The specific indicators include: ①Cobb angle of the main
curvature: the angle between the maximum angles of the two
vertebral bodies that tilt the main curvature of the spine. ②C7
Plumb Line Center Sacral Vertical Line (C7PL-CSVL): The distance between the lead line at the midpoint of the C7 vertebral
body. ③The midline of the sacrum Apical Vertebral Translation (AVT): The horizontal distance from the center of the main
curvature of the vertebral body to the midline of the sacrum.
④T1 inclination angle: the angle between the upper endplate
of the thoracic vertebral body and the horizontal line. ⑤Imaging shoulder height: The height difference of soft tissue above
the acromioclavicular joint. ⑥Sagittal Vertical Axis (SVA): The
distance between the C7 vertical line and the upper angle of
the S1 vertebral body. ⑦Thoracic Kyphosis (TK): The angle between the upper endplate of the thoracic vertebrae and the
lower endplate of the thoracic vertebrae.
Pulmonary Function Test (PFT) PFT was performed before
HPT traction, at the last traction, before internal fixation surgery, and at the last follow-up. The observation indicators included Forced Vital Capacity (FVC), the percentage of FVC measured and estimated values (FVC%), Forced Expiratory Volume
at 1 second (FEV1), and the percentage of FEV1 measured and
Estimated Values (FEV1%). To ensure the accuracy and reliability of the data, PFT was tested three times and the average value
was taken.
Statistical methods
Perform data analysis using SPSS 25.0 software. Quantitative
data that conform to normal distribution are described as (x±̄s),
and one-way repeated measures analysis of variance is used to
compare the differences in imaging indicators and lung function indicators before and after traction. Subsequently, pairwise
comparisons are conducted using Bonferroni’s test. Count data
is expressed in frequency and percentage. In repeated measures ANOVA, P<0.05 indicates a statistically significant difference; In the Bonferroni test for multiple comparisons, P<0.0125
indicates a statistically significant difference.
Results
General information of patients: Among 120 patients who
underwent HPT in the first phase, there were 40 males (33.3%)
and 80 females (66.7%); 55 cases (45.8%) were mainly characterized by kyphosis, while 65 cases (54.2%) were mainly characterized by kyphosis; Age 12-55 (32.34±13.07) years old, traction
time 5-15 (9.68±3.29)weeks, follow-up time 7-30 (19.00±6.73)
months.
All patients successfully completed the second stage simple posterior column osteotomy correction combined with
pedicle screw internal fixation, including 63 cases of thoracoplasty (52.5%) and 57 cases of combined satellite rod technology (47.5%); The surgical time was 123-400 (288.18±66.46)
minutes, and the intraoperative bleeding volume was 300-
790 (547.59±146.43) ml. There were 7-17 (12.11±3.12)
fused segments, and the height before traction was 114-158
(135.28±12.97) cm. After traction, the height was 130-165
(147.78±10.94) cm.
Comparison of imaging indicators before and after traction.
Univariate repeated measures analysis of variance showed
that there were statistically significant differences (P<0.01) in
the Cobb angle, C7PL-CSVL, AVT, T1 tilt angle, shoulder height
on imaging, SVA, TK and other indicators of the main curvature before traction, the last follow-up of traction, internal
fixation surgery, and the last follow-up of HPT treatment. The
Bonferroni pairwise comparison results showed that the imaging indicators of the patients before traction were significantly
higher than those of the last traction follow-up, internal fixation surgery, and last follow-up (P<0.01). As shown in the Table
1 below. Comparison of respiratory function indicators before
and after traction. Univariate repeated measures analysis of variance showed that there were statistically significant differences (P<0.01) in FVC, FVC%, FEV1, FEV1%, and other indicators
before traction, the last follow-up of traction, internal fixation
surgery, and the last follow-up of HPT treatment. The Bonferroni pairwise comparison results showed that the respiratory
function indicators before traction were significantly lower than
those after the last traction follow-up, internal fixation surgery,
and last follow-up (P<0.01). As shown in the Table 2.
Table 1: Comparison of imaging indicators before and after traction in 120 patients (x̄ ±s).
| Index |
Before traction |
Final traction review |
After internal fixation surgery |
Last follow-up |
F-value |
P-value |
| Cobb angle of the main curvature |
119.17±15.39 |
74.62±15.15a |
60.78±14.40a |
64.21±14.86a |
410.591 |
<0.001 |
| C7PL-CSVL(mm) |
33.33±7.21 |
13.23±4.27a |
12.42±3.58a |
12.69±3.26a |
547.127 |
<0.001 |
| AVT(mm) |
103.55±16.56 |
57.70±17.56a |
44.31±13.77a |
45.17±11.65a |
417.904 |
<0.001 |
| T1 inclination angle(°) |
20.13±5.94 |
9.29±1.73a |
8.89±2.66a |
6.51±1.77a |
397.152 |
<0.001 |
| Imaging shoulder height(mm) |
26.78±6.32 |
10.18±2.00a |
9.38±2.39a |
9.53±2.36a |
656.088 |
<0.001 |
| SVA(mm) |
38.29±5.54 |
14.41±3.24a |
17.11±3.24a |
17.50±3.07a |
968.566 |
<0.001 |
| TK(°) |
87.66±11.63 |
52.96±12.11a |
51.28±11.20a |
51.82±12.20a |
284.314 |
<0.001 |
Compared to before towing,aPτ0.01 °
Table 2: Comparison of respiratory function indicators before and after traction in 120 patients (x̄ ±s).
| Index |
Before traction |
Final traction review |
After internal fixation surgery |
Last follow-up |
F-value |
P-value |
| FVC(L) |
1.13±0.19 |
1.36±0.28a |
1.49±0.28a |
1.53±0.26a |
57.608 |
<0.001 |
| FVC% |
31.61±4.64 |
36.19±4.95a |
38.08±7.46a |
38.61±6.91a |
32.188 |
<0.001 |
| FEV1(L) |
1.08±0.22 |
1.17±0.19a |
1.26±0.22a |
1.28±0.24a |
20.670 |
<0.001 |
| FEV1% |
29.68±11.56 |
33.45±5.97a |
35.91±7.81a |
36.88±7.85a |
16.550 |
<0.001 |
Compared to before towing,aP<0.01。
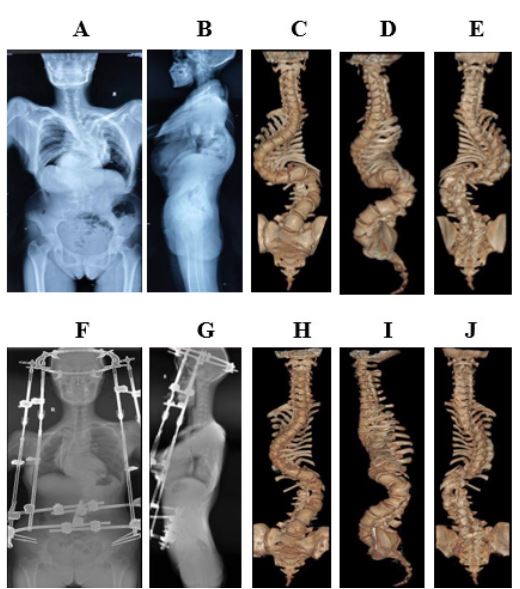
Introduction to typical cases
Patient Zhang, female, 25 years old. Upon admission, X-ray
examination diagnosed scoliosis, kyphosis, Marfan syndrome,
and pulmonary insufficiency. Preoperatively, the entire spine
was displayed in both the anterior and lateral positions, with
scoliosis (S) and thoracic deformities, as shown in Figure 1 (AB); Preoperative 3D imaging of the entire spine showed scoliosis in an “S” shape, with some vertebral bodies showing poor
segmentation and deformities in the chest and ribs, as shown
in Figure 1 (C-E). After 3 months of improved HPT treatment,
the entire spine was displayed in both the anterior and lateral
positions, and there was a significant improvement in scoliosis
compared to before, as shown in Figure 1 (F-G); The 3D imaging
of the entire spine shows significant improvement in scoliosis,
as well as chest and rib deformities, as shown in Figure 1 (H-J).
Discussion
Traditional HPT applications are not widely used, mainly
due to inconvenient installation of HPT traction devices, low
fault tolerance, and poor patient tolerance. Hai Yong [11] believes that although HPT can correct various spinal deformities
through strong traction, due to the connecting rod surrounding
the body and fixed position, it is difficult to avoid some spinal
deformities. Even if it is reluctantly installed, it will compress
the local skin and affect the traction effect. This study used
modified HPT traction therapy for patients with severe spinal
deformities and respiratory dysfunction. The results showed
that all imaging indicators of patients after traction (last followup, internal fixation surgery, and last follow-up) were lower
than before traction, indicating that modified HPT traction has
significantly restored overall balance in the coronal and sagittal
planes, as well as local balance in the shoulder and pelvis. This
is because traditional HPT is cumbersome to wear and does not
allow patients to sleep on their backs, making it impossible to
perform traction around the clock. The improved HPT traction
rod placed on the front and outer sides of the body can effectively avoid spinal deformities, allowing patients to sleep and
dress in a supine position. It can achieve 24-hour continuous
traction and provide strong traction all day, effectively correcting spinal deformities. In addition, the traditional HPT structure
is relatively single, and due to differences in patient body size,
personalized traction cannot be achieved. The improved pelvic ring of HPT is a half ring, which can be worn from the side,
avoiding the inconvenience caused by the traditional HPT pelvic
closed-loop structure being worn from the foot. At the same
time, the semi-circular structure can adjust its size and shape,
suitable for patients of different body types, thereby effectively
improving traction efficiency and improving spinal deformities.
Qi et al. [12] reported that the combination of HPT and spinal
release surgery can improve traction, but according to the author’s report, the average corrected Cobb angle for patients after surgery is about 38.5°, slightly lower than the results of this
study. However, it should be pointed out that there are obvious
shortcomings in simply pursuing traction efficiency and combining spinal release surgery. Spinal release surgery can increase
surgical trauma and treatment costs, while also increasing the
incidence of cardiovascular and pulmonary complications [13].
Sui Wenyuan et al. [14] also confirmed that rapid correction of
severe spinal deformities with respiratory dysfunction not only
fails to achieve the expected results, but also increases the risk
of complications and mortality. Relatively speaking, improved
HPT can provide strong traction and continuously act on the
main curvature area of the spine, gradually improving body balance and spinal sequence, avoiding the risk of nerve damage
and complications caused by violent correction. At the same
time, it can also increase patient tolerance and improve comfort through relatively free positioning and convenient wearing
methods.
Severe spinal deformities not only affect the appearance of
patients, but when deformities occur in the thoracic vertebrae,
they can cause chest collapse, spinal shortening, reduced thoracic volume, and lead to pulmonary ventilation dysfunction.
However, rapid correction is not recommended for patients with
severe spinal deformities and respiratory dysfunction, as violent
correction can increase the risk of nerve damage, disability, and
mortality [15]. The results of this study showed that the respiratory function indicators at each stage after using modified HPT
traction were significantly better than before traction, indicating that modified HPT treatment can improve the respiratory
function of patients. This is because the improved HPT adopts
a relatively mild adjustment method, which achieves the purpose of traction and correction of spinal deformities by intermittently adjusting the traction frame, thereby alleviating the
compression of the spine on the thoracic cavity. Liu Dun et al.
[16] believe that although HGT can improve respiratory function in patients with severe spinal deformities, it is only suitable for young children with good flexibility in severe spinal
deformities, and its effect on severe stiff spinal deformities and
middle-aged and elderly patients is poor. The improved HPT
uses a connecting rod between the pelvic ring and the halo ring
to traction the spine, providing stable and sustainable traction
without affecting patient cardiovascular exercise. The improved
HPT also has the characteristics of controllability and gradual
progression, with high safety. It avoids strong stimulation to
the heart and lungs while slowly pulling the spine. As the spine
height is elongated and the chest is formed, the corresponding chest deformity and volume are significantly improved, and
the patient’s lung function is also significantly improved. This
study also found that the trend of respiratory function changes
in patients gradually improved over time, indicating that HPT
traction therapy promotes thoracic remodeling and gradually
improves anterograde thoracic compliance. At the same time,
HPT slow stretching of the spine is improved to match respiratory muscles with thoracic volume, and ventilation function
gradually improves. Improved HPT can not only be used for
preoperative correction of spinal deformities, but also for maintaining traction during surgery and facilitating the placement of
internal fixation devices, as the traction frame is placed on the
anterior lateral side, promoting patient recovery. Qi et al. [17]
also believe that for patients who are unable to install purely
mechanically and have difficulty with internal fixation, HPT traction can reduce the difficulty of internal fixation installation,
reduce load, and effectively prevent the risk of decoupling and
rod breakage. It is an effective auxiliary treatment measure for
severe spinal deformities.
Conclusion
In summary, the improved HPT traction treatment for patients with severe spinal deformities and respiratory dysfunction can effectively correct spinal deformities, restore overall
spinal balance, and improve respiratory function. It is a safe and
effective auxiliary treatment measure for severe spinal deformities and respiratory dysfunction. There are the following shortcomings in this study: ①The included cases were all patients
who underwent HPT treatment in the first stage and underwent
corrective surgery in the second stage. Due to the inability of
patients whose respiratory function did not meet the requirements after traction to undergo the second stage surgery, this
study can only reflect cases of patients with significant HPT
treatment effects. ②During the last follow-up pulmonary function test, the patient’s spine was still in a fixed state, and the
patient’s forced breathing range was limited, which may affect the results of respiratory function indicators. In future research,
we will conduct in-depth analysis of the relationship between
the duration and timeliness of traction therapy, aiming to optimize the treatment process and improve traction efficiency of
improved HPT. At the same time, we will also consider introducing comfort indicators to better promote the application of
improved HPT.
References
- Garg B, Mehta N. Modified posterior vertebral column resection for severe spinal deformity: a retrospective, comparative study[J]. Spine J. 2020; 20(9): 1446-1451. DOI: 10.1016/j.spinee.2020.04.014.
- Jagger F, Tsirikos AI, Blacklock S, et al. Adaptation to reduced lung function in children and young people with spinal deformity [J]. J Clin Orthop Trauma. 2020; 11(2): 191-195. DOI: 10.1016/j.jcot.2019.12.013.
- Lin S, Ma S, Zhou Z, et al. Improvement of pulmonary function and reconstructed 3D lung volume after deformity correction for thoracic spinal posttubercular kyphosis: A multicenter study [J]. J Neurosurg Spine. 2023; 39(1): 58-64. DOI: 10.3171/2023.3.SPINE221382.
- Wang Lihang, Chen Qiling, Lu Tingsheng, et al. The significance of using head pelvic ring traction to correct severe stiff spinal deformities [J]. Chinese Journal of Orthopedics, 2022; 30(18): 1704-1707. DOI:10.3977/j.issn.1005-8478.2022.18.16.
- Hu M, Lai A, Zhang Z, et al. Intraoperative halo-femoral traction during posterior spinal arthrodesis for adolescent idiopathic scoliosis curves between 70° and 100°: A randomized controlled trial [J]. J Neurosurg Spine. 2021; 36(1): 78-85. DOI: 10.3171/2021.2.SPINE21184.
- Shi Benlong, Li Yang, Liu Zhen, et al. Application of Halo gravity traction before corrective surgery for severe upper thoracic angular kyphosis with nerve damage [J]. Chinese Journal of Orthopedics. 2021; 41(7): 412-419. DOI:10.3760/cma.j.cn121113-20200818-00508.
- Sun Y, Zhang Y, Ma H, et al. Halo-pelvic traction in the treatment of severe scoliosis: a meta-analysis [J]. Eur Spine J. 2023; 32(3): 874-882. DOI: 10.1007/s00586-023-07525-7.
- Zhang Yushuang, Equation, Huang Lijun, et al. Clinical effects of applying Halo pelvic traction in the treatment of severe stiff spinal deformities in adults [J]. Journal of Orthopedic Clinical and Research. 2021; 6(6): 340-345. DOI:10.19548/j.2096-269x.2021.06.005.
- McIntosh AL, Ramo BS, Johnston CE. Halo Gravity Traction for Severe Pediatric Spinal Deformity: A Clinical Concepts Review [J]. Spine Deform. 2019; 7(3): 395-403. DOI: 10.1016/j.jspd.2018.09.068.
- Yang C, Wang H, Zheng Z, et al. Halo-gravity traction in the treatment of severe spinal deformity: a systematic review and metaanalysis [J]. Eur Spine J. 2017; 26(7): 1810-1816. DOI: 10.1007/s00586-016-4848-y.
- Hai Yong. Development History of Spinal Surgery in China [J]. Chinese Journal of Orthopedics and Arthrology. 2019; 8(10): 721-725. DOI:10.3969/j.issn.2095-252X.2019.10.001.
- Qi L, Xu B, Li C, et al. Clinical efficacy of short-term pre-operative halo-pelvic traction in the treatment of severe spinal deformities complicated with respiratory dysfunction [J]. BMC Musculoskelet Disord. 2020; 21(1): 665. DOI: 10.1186/s12891-020-03700-9.
- Du Ping, Xu Huaye, Zhu Huijie, et al. Study on the effect of red blood cell suspension pre washing method in preventing hyperkalemia during pediatric scoliosis correction surgery [J]. Chinese Journal of Physician Continuing Education. 2020; 43(11): 969-972. DOI:10.3760/cma.j.cn115455-20200513-00607.
- Sui Wenyuan, Liu Hanzhong, Zhang Wei, et al. The effect of Halo gravity traction on lung function in adolescent patients with severe stiff spinal deformities accompanied by respiratory dysfunction [J]. Chinese Journal of Orthopedic and Joint Surgery. 2019; 12(1): 30-34. DOI:10.3969/j.issn.2095-9958.2019.01.007.
- Wang J, Han B, Hai Y, et al. How helpful is the halo-gravity traction in severe spinal deformity patients?: A systematic review and meta-analysis [J]. Eur Spine J. 2021; 30(11): 3162-3171. DOI: 10.1007/s00586-021-06902-4.
- Liu Dun, Li Yang, Shi Benlong, et al. Application of Halo gravity traction in patients with type I neurofibromatosis and severe scoliosis [J]. Chinese Journal of Surgery, 2019; 57(2): 119-123. DOI:10.3760/cma.j.issn.0529-5815.2019.02.009.
- Qi L, Zhao Y, Xu B, et al. Two-stage treatment for severe spinal kyphotic deformity secondary to tuberculosis: halo-pelvic traction followed by a posterior-only approach correction [J]. BMC Musculoskelet Disord. 2022; 23(1): 991. DOI:10.1186/s12891-022-05974-7.