Introduction
Testicular implants have been in use since 1941. They have
been available for patients with various conditions resulting in
absence of testicles in the scrotum, such as testicular atrophy
and orchidectomy, in order to minimize psychological distress
and to improve cosmetic outcomes [1,2].
The quality of testicular prostheses has improved considerably over time, however, there remains risks associated with
these implants. Testicular prosthesis rupture is very rare, contrary to breast implants rupture [2].
We report on a rare case of granulomatous scrotal lesion
suspicious of malignancy most likely due to a chronic testicular prosthesis leak which may be caused by repeated chronic
trauma (cycling).
Case presentation
A 54-year-old male presented to the urology clinic with right
scrotal pain and swelling. He has a history of bilateral testicular
atrophy in childhood and bilateral testicular prosthesis placement at age of 14 years without orchidectomy and has been
on testosterone replacement since then. He denied any scrotal
trauma but he is a keen cyclist.
Clinically, he had a small and firm lump in the lower part of
the right scrotum. Both testicular prostheses were palpable and
in good position in the scrotum. Blood and urine tests including
AFP, Beta-HCG, LDH, and PSA were unremarkable. Scrotal Ultrasound showed bilateral testicular prosthesis, normal in position
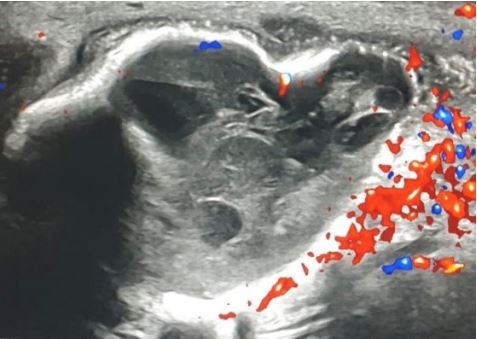
and in consistency. In the right scrotal area, there was a heterogenous solid cystic mass, inferior and medial to the lower pole of the testicular prosthesis, with no internal vascularity, possibly sinister given the history of testicular atrophy (Figure 1).
We arranged scrotal and pelvic MRI with contrast which revealed oblong space-occupying lesion measuring 3 cm, with
significant internal enhancement, indenting the inferomedial
aspect of the right prosthesis (Figure 2). This mass had features
suggestive of a chronic process such as a granuloma, however
due to atypical features, it was difficult to exclude a malignant
process. In view of low suspicion of malignancy, we arranged
CT chest, abdomen, and pelvis with contrast, which showed no
abnormalities.
Right scrotal exploration, with removal of the right testicular
prosthesis and excision of the fibrous capsule and right scrotal cystic lesion was performed. The prosthesis appeared deformed with loss of volume, suggestive of chronic leak, likely
from the lower pole fixation point (Figure 3). The right atrophic
testis was seen in the upper part of the right scrotum and right
orchidectomy was performed.
Histology of the excised cystic structure and fibrous capsule
confirmed haemorrhagic granulomatous tissue, surrounded by
fibrin. Interestingly, histology of the excised testis confirmed
atrophic testicular tissue with granulomatous inflammation and
foreign-body type giant cells in the tunica vaginalis and spermatic cord (Figure 4). There was no evidence of malignancy in
either cystic lesion or the atrophic testis.
Discussion
Complications of silicone gel testicular prosthesis include
rupture of the prosthesis, scrotal contraction, migration into
the inguinal canal, infection, pain, and rarely haematoma. Immune complications have also been documented [3]. Testicular
silicone prosthesis rupture is a rare event in clinical practice,
compared to breast silicone prostheses [1]. The scrotum offers
more mobility, low tension position and low temperature, making them potentially less vulnerable to pressure injury [4].
We identified 9 cases of spontaneous testicular prosthesis
rupture, reported in the English literature; most of which were
not associated with trauma [1-5]. Spontaneous rupture of the
silicone prosthesis was more commonly described as intra-fibrous capsule rupture [1-4]. We describe a granulomatous scrotal mass at the lower part of the testicular prosthesis. The prosthesis had a deformed shape, likely due to small chronic leakage
which may cause by repeated chronic trauma (cycling). The fibrous prosthesis capsule was intact, however the histological
findings of the atrophic testicular tissue with granulomatous inflammation and foreign-body type giant cells in the tunica vaginalis and spermatic cord, may suggest extra-capsular silicone
migration. Similarly, others noted trans-capsular migration of
silicone particles, even when the fibrous capsule was intact [1].
Previously documented intervals between placement of the
prosthesis and removal due to rupture ranged between twelve
and seventeen years [3,5]. In our case the patient had his testicular prosthesis 40 years prior to the exploration and removal
of the prosthesis. To our knowledge, this is the longest period
between insertion of testicular prosthesis and removal due to
complications of the prosthesis.
The assessment of testicular prosthesis spontaneous rupture
is based on clinical examination and on imaging findings seen
on ultrasound in most of the cases. The “stepladder” sign seen
on US occurs when silicone gel causes the elastomer shell to
fold on itself and produce thin echogenic lines coursing parallel
to the ultrasound probe surface [2]. In our case there were no
ultrasound signs of prosthesis rupture as the prosthesis looked
normal in position and consistency. The lack of the stepladder
sign may be due to a small volume of silicone leak in our case.
MRI imaging offers superior diagnostic accuracy, usually
demonstrating the Linguini sign with multiple curvilinear hypointense lines within the ruptured implant high signal intensity silicone filling [4]. In our case, the MRI did not demonstrate
the linguini sign and showed signs suggestive of a granulomatous mass but did not rule out malignancy.
The prosthesis should be removed if rupture is suspected, to
prevent the development of local inflammatory changes of the
surrounding tissue and regional lymph nodes [2]. In our case
we removed the testicular prosthesis and excised the scrotal
mass due to the scrotal pain and low suspicion of possible malignancy.
Conclusion
Spontaneous silicone leaks from testicular prosthesis are
rare. In our case there were no typical radiological findings of a
prosthesis leak on either US or MRI. Therefore, scrotal exploration and removal of the deformed prosthesis was necessary to
reach a diagnosis and definitive treatment.
Declarations
Consent: The director of the study obtained a verbal consent
from the patient to publish this case report.
Conflict of interest statement: We declare that all authors
have no financial and personal relationships with other people
or organizations that could inappropriately influence (bias) this
work.
References
- Quang-Bao Phan, Nicolas Koutlidis, Céline Duperron, Eric
Mourey, Frédéric Michel, et al. Case reports in urology. Management of Testicular Silicone Gel-Filled Prosthesis Rupture: Case
Report of a Rare Event and a Review of the Literature. 2016.
10.1155/2016/2824802.
- Sonali Ranjit, Rebecca Dameron, Ayman Mithqal. Urology Case
Reports. Spontaneous testicular silicone prosthesis rupture, a
rare event. 2021; 37. 10.1016/j.eucr.2021.101626.
- Michael St J Floyd, Helen Williams, Sanjay K Agarwal, Alan R De
Bolla. Journal of Medical Case Reports. Unilateral spontaneous
rupture of a testicular implant thirteen years after bilateral insertion: A case report. 2010. 10.1186/1752-1947-4-341.
- J J Hage, A H Taets van Amerongen, P J Van Diest. Journal of Urology. Rupture of silicone gel filled testicular prosthesis: Causes,
diagnostic modalities and treatment of a rare event. 1999.
10.1016/s0022-5347(01)61925-6.
- TT John, MVP Fordham. Journal of Urology. Spontaneous rupture of testicular prosthesis with external leakage of silicone-a
rare event. 2003. 10.1097/01.ju.0000087615. 35085.c9