Introduction
Hyperlactatemia is defined as elevations in blood lactate >2
mmol above baseline without concurrent metabolic acidosis
[1]. Prolonged hyperlactatemia can be an independent risk factor for worse outcomes as lactate is a byproduct of anaerobic
metabolism and linked with tissue ischemia and/or organ dysfunction.
In head and neck surgical patients, normalization of hyperlactatemia is crucial to decrease mortality and postoperative
complications [2]. However, even in critically-ill surgical patients,
hyperlactatemia is not necessarily indicative of circulatory failure [3]. Our center has anecdotally noted hyperlactatemia in
patients undergoing Facial Gender-Affirmation Surgery (FGAS),
but it remains unclear whether it corresponds directly to adverse clinical outcomes. The present study sought to examine
implications of intraoperative hyperlactatemia during FGAS.
Methods
Patients and procedures
The Institutional Review Board at the University of California,
San Francisco (UCSF) approved this retrospective analysis of the
UCSF Gender-affirming Facial Plastic Surgery Database. Patient
consent was not required for this study which included deidentified patient data and was observational in nature. Inclusion criteria were patients >18 years undergoing FGAS between
2015-2023 with documented intraoperative lactate levels. Exclusion criteria were patients <18 years or no documented intraoperative lactate levels.
Data collection
Data collected included age, procedures, duration, estimated blood loss, complications, transfusions, and perioperative
fluid volume.
Data analysis
Primary outcome measures were peak lactate level and time
to normalization (<2 mmol/L). Lactate levels and time points
were plotted over time to create a trend graph. Data was extrapolated from a descriptive table to determine average ages,
durations of surgery, estimated blood loss, volume resuscitation
and lactate levels.
Results
Of 130 patients evaluated, 17 met inclusion criteria, all of
whom underwent comprehensive facial gender affirmation surgery. All patients analyzed were assigned males at birth who underwent facial feminization surgeries. Procedures included frontal bone contouring/cranioplasty, hairline advancement, brow,
face, and neck lift, cheek and lip augmentation, rhinoplasty, alar base reduction, mandibular contouring, neck liposuction, chondrolaryngoplasty, and earlobe reduction. The average age of
patients was 35. All 17 patients were on estradiol therapy with
doses ranging from 1 mg oral daily to 40 mg/ml injections every
14 days. 4/17 patients held their estrogen medication 2 weeks
prior to surgery. On average, surgeries lasted 710 minutes (95%
Confidence Interval (CI): 650, 770) had an estimated blood loss
of 427 mL (95% CI: 288, 567) (Table 1) and intraoperative fluid
volume resuscitation of 2752 mL (95% CI: 1935, 3570) (Table
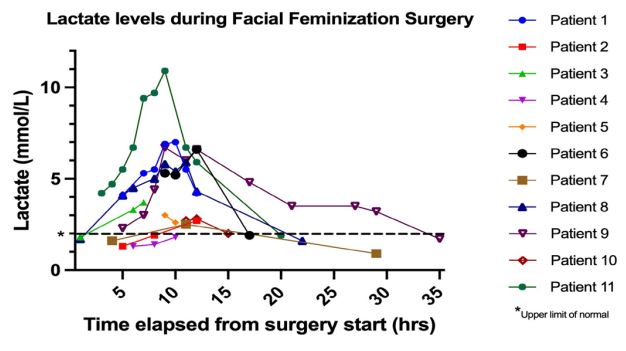
2). Intraoperative lactate levels ranged from 1.2-10.9 mmol/L
with mean value of 3.8 (95% CI: 2.2, 5.4) (Figure 1). Nearly every
patient demonstrated peak lactate around the end of surgery
(~10h) with normalization by postoperative day one.
Table 1: Characteristics of patients undergoing facial gender affirmation surgery.
| Patient |
Age |
Surgery duration (mins) |
Blood loss (mL) |
Peak lactate level (mmol) |
Length of hospital stay (days) |
| 1 |
46 |
679 |
800 |
7 |
2 |
| 2 |
62 |
606 |
500 |
2.7 |
2 |
| 3 |
38 |
770 |
300 |
3.7 |
1 |
| 4 |
30 |
716 |
300 |
2 |
1 |
| 5 |
30 |
656 |
870 |
1.8 |
3 |
| 6 |
50 |
778 |
300 |
3 |
1 |
| 7 |
26 |
780 |
500 |
1.2 |
2 |
| 8 |
26 |
717 |
200 |
3.9 |
1 |
| 9 |
29 |
690 |
250 |
1.9 |
1 |
| 10 |
25 |
731 |
300 |
5.3 |
1 |
| 11 |
31 |
653 |
300 |
6.7 |
3 |
| 12 |
23 |
376a |
800 |
2.5 |
3 |
| 13 |
33 |
943 |
350 |
2.8 |
3 |
| 14 |
30 |
671 |
200 |
10.9 |
4 |
| 15 |
33 |
721 |
500 |
5.9 |
1 |
| 16 |
43 |
490 |
200 |
1.4 |
4 |
| 17 |
46 |
767 |
600 |
1.8 |
1 |
Table 2: Fluid resuscitation for patients undergoing facial gender affirmation surgery.
| Patient |
RBC (mL) |
Intraoperative fluids |
Postoperative fluids |
|
|
PE (mcg) |
Ephedrine (mg) |
TXA (mg) |
NE (mcg) |
PL (mL) |
Albumin (mL) |
LR (mL) |
NS (mL) |
LR
(mL) |
PL (mL) |
5% Dextrose, 0.9
NaCl (mL) |
| 1 |
|
4335 |
12.5 |
|
|
|
|
|
|
|
3000 |
|
| 2 |
|
6200 |
|
|
|
|
|
|
|
|
|
550 |
| 3 |
|
29780 |
25 |
|
|
|
|
|
|
375 |
|
|
| 4 |
|
12485 |
|
|
|
|
500 |
|
|
1200 |
|
|
| 5 |
307 |
10475 |
|
|
|
1700 |
500 |
|
|
|
|
350 |
| 6 |
|
4765 |
|
1738.4 |
|
|
1000 |
3000 |
|
60 |
|
1000 |
| 7 |
|
11850 |
|
1179 |
|
|
|
1800 |
500 |
|
|
|
| 8 |
|
7635 |
|
1013 |
21.458 |
|
|
3000 |
500 |
1500 |
|
|
| 9 |
|
11920 |
|
1405 |
|
|
500 |
2500 |
|
|
|
|
| 10 |
|
11020 |
|
|
|
|
|
3850 |
500 |
|
300 |
|
| 11 |
350 |
12055 |
40 |
1405.4 |
16 |
4000 |
|
2500 |
500 |
180 |
500 |
900 |
| 12 |
700 |
17595 |
|
710 |
16.65 |
|
|
2750 |
|
|
|
|
| 13 |
|
14875 |
|
1292 |
|
|
|
2000 |
|
2700 |
500 |
|
| 14 |
350 |
|
30 |
1298 |
|
|
|
5000 |
700 |
|
|
|
| 15 |
|
14545 |
|
|
1.511 |
1900 |
2000 |
1800 |
|
|
|
|
| 16 |
|
14520 |
|
848 |
|
|
|
|
|
|
|
|
| 17 |
|
23495 |
15 |
1491.9 |
|
|
|
3200 |
600 |
|
|
|
Patient intraoperative and post-operative fluid requirements.
TXA: Tranexamic Acid; NS: Normal Saline; LR: Lactated Ringers; RBC: Red Blood Cell Transfusion; PL: Plasmalyte; NE: Norepinephrine; PE: Phen-
ylephrine
Discussion
To our knowledge, no studies exist examining intraoperative lactatemia during FGAS. Normalization of intraoperative
lactatemia could be explained by similar trends seen in head
and neck surgeries [4]. During reconstructive head and neck
surgery, intraoperative lactatemia was not influenced by vasopressors or blood transfusions, and typically normalized by 24
hours postoperatively [5]. In the present study, all patients were
treated with intraoperative fluids and/or red blood cell transfusion with subsequent resolution of lactatemia, although a direct
correlation between the two could not be made.
We speculate the etiology of lactatemia in FGAS patients
may be due to influences of estrogen therapy superimposed
on intraoperative hypoperfusion or physiologic stress response.
Higher plasma lactate levels have been described in biological
females with higher estradiol levels [4], and may be associated
with exogenous administration. The peak around 10-12h in our
data corresponds with the average duration of 11.8h (710 min)
suggesting that downtrending began upon procedure completion, cessation of blood loss, and surgical closure.
Limitations
Selection bias was a limitation; only patients with documented intraoperative lactate levels, typically drawn at the discretion
of the anesthesiologist based on patient hemodynamic status,
were included. Blood loss was estimated rather than measured
which allowed for variability in reported data points. Though
most patients underwent similar procedures, there was variability in the specific permutation of maneuvers performed.
Conclusion
In our study, intraoperative lactatemia was transient and
normalized during the surgery or shortly thereafter. Given these
findings, we cautiously conclude that intraoperative lactatemia
during facial gender affirmation surgery may be managed expectantly in the absence of end-organ damage or clinical deterioration.
Keypoints
The impact of hyperlactatemia following Facial Gender Affirmation Surgery (FGAS) remains unclear. The present study
sought to examine implications of intraoperative hyperlactatemia during FGAS.
This retrospective cohort study included patients undergoing
FGAS between 2015 and 2023 with at least two intraoperative
lactate levels. Intraoperative lactate levels were plotted against
surgery duration.
The study included 17 patients with peak lactate levels ranging from 1.2-10.9 mmol/L. Lactate levels normalized by the end
of surgery or on the first postoperative day.
This study highlights the reassuring lactate normalization
within one day of surgery. We cautiously conclude that intraoperative lactatemia may be managed expectantly.
Declarations
Study design: Retrospective cohort study.
Data sharing & data availability: The authors confirm that
the data supporting the findings of this study are available within the article. Raw data that support the findings of this study
are available upon reasonable request.
Author’s contributions: AS: Conception, Methodology, Writing. RMB: Conception, Methodology, Data Analysis, Writing.
SM: Conception, Methodology, Data Analysis, Writing. AP: Writing, Editing. PDK: Writing, Editing. RS: Writing, Editing.
Acknowledgements: None.
Author disclosure statement: None of the authors have any
relevant conflicts of interest or disclosures to make.
Funding information: There were no funding sources for this
project.
References
- Godinjak A, Jusufovic S, Rama A, et al. Hyperlactatemia
and the importance of repeated lactate measurements in
critically ill patients. Med Arch. 2017; 71(6): 404-407; doi:
10.5455/medarh.2017.71.404-407.
- Souza SP, Serra MG, Oliveira NDS, et al. Arterial lactate as a
predictor of postoperative complications in head and neck
squamous cell carcinoma. Braz J Otorhinolaryngol. 2022;
88 (Suppl 1): S97-S101; doi: 10.1016/j.bjorl.2021.04.008.
- Bakker J, de Lima AP. Increased blood lactate levels: an
important warning signal in surgical practice. Crit Care.
2004; 8(2): 96-98; doi: 10.1186/cc2841.
- Shen Y, Liu F, Li Q, et al. The gonadal hormone regulates
the plasma lactate levels in type 2 diabetes treated with
and without metformin. Diabetes Technol Ther. 2012;
14(6): 469-474; doi: 10.1089/dia.2011.0275.
- Roy PM, Bharti K, Sinha S, et al. Acute perioperative hyperlactatemia in oncoplastic reconstructive surgeries:
What is the significance? J Anaesthesiol Clin Pharmacol.
2021; 37(3): 416-418; doi: 10.4103/joacp.JOACP_297_19.