Introduction
The Internal Jugular Vein Catheter (IJC) plays a crucial role
in the management of patients with kidney failure who necessitate Hemodialysis (HD). Internal Jugular Vein (IJV) catheterization is commonly used to obtain HD access in patients with
renal failure, and it is associated with a high rate of successful
catheter placement. Significant complications such as carotid
artery puncture, vessel erosion, pneumothorax, airway obstruction, thrombosis, and infection can occur during this procedure.
Multiple catheter placements may be required for HD patients.
This, combined with their comorbid conditions, raises the likelihood of such complications [1,2]. We present a case of an HD
patient who developed an unusual complication of localized alveolar hemorrhage after left IJV catheterization.
Case presentation
Case of 66 years old, female patient, smoker, known to have
hypertension, old stroke without sequalae, Chronic Obstructive
Pulmonary Disease (COPD), end stage renal disease recently
started on hemodialysis via intermittent right internal jugular
catheter, waiting right arm arteriovenous fistula presented with
non-functional right catheter, admitted for replacement of the
dialysis catheter. A left internal jugular dialysis catheter was inserted after multiple attempts. After 1 hour, patient started to
have minimal hemoptysis, chest discomfort and dyspnea at rest
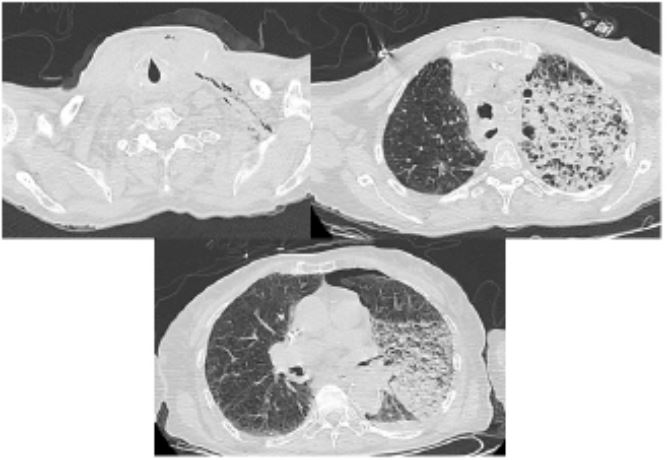
with increase oxygen requirement. A Computer Tomography
(CT) scan of chest was conducted, showing left minimal pneumothorax, left neck subcutaneous emphysema, and left upper
lobe infiltrates suggestive of alveolar hemorrhage (Figure 1).
A CT with intravenous contrast was performed, after 24
hours, didn’t revealed any source of bleeding. A non-rebreather
face mask was applied to patient delivering 15 l/min O2
, ethamsylate (Dicynone) 500 mg every 8 hours was started, intravenous broad spectrum antibiotics with steroids were given and
patient was transferred to Intensive Care Unit (ICU) for close
monitoring. After 2 days, patient improved and was transferred
to floor without any oxygen requirement. Thereafter she was
discharged home.
Discussion
Each year, approximately five million Central Venous Catheters (CVCs) are implanted in the United States. Infectious complications are reported in 5% to 26% of CVC patients, thrombotic complications in 2% to 26%, and mechanical complications in
5% to 19%. The most common mechanical complications during
CVC insertion are pneumothorax, hematoma, arterial puncture,
and line misplacement. They are more common with less experience or after three attempts. Air embolism, arterial laceration,
arrhythmia, hydrothorax, and superior vena cava perforation
have all been reported as potentially fatal complications [3].
Hemoptysis is a rare complication of IJV puncture in the setting of central venous catheterization, with only a few cases
reported in the literature to the best of our knowledge. It was
difficult to determine the precise mechanism of lung injury in
this case [4].
Friedman et al. [5] described massive hemoptysis during IJV
cannulation, which was associated with airway obstruction and
a cervical hematoma, but did not specify the underlying mechanism. A needle-created fistulous tract between the IJV, carotid
artery, and trachea is one possible mechanism. Wiseheart et
al. [6] also reported a massive hemorrhage following IJV catheterization, which eventually led to death. This was caused by a
secondary hemothorax caused by tears in the mediastinal and
apical pleura following an ascending cervical artery puncture.
Localized alveolar hemorrhage can occur as a result of excessive bronchial circulation bleeding, which can swiftly inundate
the alveoli [3]. One possible explanation is that the guide wire
becomes trapped against the vessel wall during insertion, and
subsequent insertion of the dilator or catheter causes the wire to bend and push against the vessel wall [7]. This can result in
a laceration injury. A direct visualization of the guide wire using
ultrasound or fluoroscopy can help to prevent atria or venous
injury.
In this case, the placement of a left internal jugular vein line
coincided with hemoptysis and the development of a left upper
lobe infiltrate. Although significant bleeding was not visible on
angiogram, we hypothesize that one or more perforations of
the bronchial artery caused the alveolar hemorrhage in the left
upper lobe.
Pneumothoraxes occur in about 1% of cases and are most
frequently seen with subclavian vein central lines. Any injury to
the parietal pleura during insertion will result in pneumomediastinum or pneumothorax formation. A greater number of attempted insertions and a larger catheter size increase the risk
of pneumothorax [8].
Tsotsolis et al. [9] concluded that ultrasound guidance catheterization reduces the number of catheter placement failures,
the time required for IJV insertion, and mechanical complications.
Conclusion
The sudden occurrence of severe hemoptysis and pneumothorax during the insertion of an IJV catheter emphasizes the
potentially life-threatening complications in this case report.
Additional precautions, such as the use of ultrasound and fluoroscopy guidance catheterization, should be taken to avoid
complications. Catheter should be inserted by experienced
hands, with no force applied while passing the guidewire, dilators, and catheter itself.
Declarations
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and
any accompanying images. A copy of the written consent is
available for review upon request by the Editor-in-Chief of this
journal.
Ethics approval and consent to participate: Ethical approval
was not applicable.
Conflict of interest: The authors declare that they have no
conflict of interest.
Financial disclosure: The authors declared that this study
has received no financial support.
Authors’ contributions: Shereen Mollaei (SM) contributed
to the diagnosis and management of the case. Zeinab El Mawla
(ZM) contributed to the conceptualization and planning of the
case report. ZM provided the preparation of manuscript. Both
authors read and approved the final manuscript.
Acknowledgments: Not applicable.
References
- Cho, Elizabeth MD, Mcgoldrick KEM. Injuries And Liability Related To Central Vascular Catheters A Closed Claims Analysis. Surv Anesthesiol. 2005; 49(3): 154-155. Doi:10.1097/01.Sa.0000165245.45492.1c
- Deepak K Tempe, Sanjula Virmani, Jyotsna Agarwal, Manisha Hemrajani, Subodh Satyarthy HSM. The Success Rate And Safety Of Internal Jugular Vein Cannulation Using Anatomical Landmark Technique In Patients Undergoing Cardiothoracic Surgery. Ann Card Anaesth. 2013; 16(1): 16-20. Doi:10.4103/0971-9784.105364
- Bawa AS, Jain V, Gutierrez G. Local pulmonary hemorrhage as a complication of subclavian vein catheterization. Chest. 2007; 132(4): 695A. Doi:10.1378/Chest.132.4
- Johari HG, Lashkarizadeh MM, Mardani P, Shahriarirad R. Massive Hemoptysis Following Cannulation Of Right Internal Jugular Vein For Insertion Of Cuffed Hemodialysis Catheter: A Rare Complication Of Central Venous Catheterization. 2021. Doi:10.1177/1129729820910304
- Y Friedman, E Tilly, E C Rackow MHW. Massive Hemoptysis During Catheterization of the Internal Jugular Vein. Chest. 1989; 95(5): 1143. Doi:10.1378/Chest.95.5.1143
- Wisheart JD, Hassan MA, Jackson JW. A Complication Of Percutaneous Cannulation of the Internal Jugular Vein. 1972; 496-499.
- Craig Kornbau, Kathryn C Lee, Gwendolyn D Hughes, MSF. Central Line Complications. Int J Crit Illn Inj Sci. 2015; 5(3): 170-178. Doi:10.4103/2229-5151.164940
- Sadaf T, Bhutta M, William C, Culp M. Evaluation And Management of Central Venous Access Complications. Tech Vasc Interv Radiol. 2011; 14. Doi:Https://Doi.Org/10.1053/J.Tvir.2011.05.003
- Tsotsolis N, Tsirgogianni K, Kioumis I, et al. Pneumothorax As A Complication of Central Venous Catheter Insertion. 2015; 3(3): 1-10. Doi:10.3978/J.Issn.2305-5839.2015.02.11.