Introduction
Intussusception, the invagination of a part of the bowel into
the adjacent segment, affects both children and adults [1]. However, the aetiology, clinical features and management of adult
intussusception are quite different from the paediatric disease
[2]. Intussusception represents only about 1% of bowel obstruction in the adult population, 0.08% of all abdominal operations
and < 0.1% of overall hospital admissions among adults [3].
Unlike childhood intussusception, the adult condition rarely presents with the classical triad of colicky abdominal pain,
abdominal lump and the passage of red currant jelly stool [4].
Indeed, the clinical presentation of intussusception in adults is
often ambiguous, elusive and nonspecific, thereby making the
diagnosis very challenging [5]. This is because adult intussusception is an infrequent cause of abdominal pain and intestinal
obstruction. Likewise, the clinical examination of these patients
is often negative. However, meticulous clinical history and physical examination combined with ancillary imaging investigations,
like abdominal ultrasound scan and Multi-Detector Computed
Tomography (MDCT) scan, readily provide the accurate diagnosis in the adult patient [6].
Whereas the uncomplicated childhood intussusception
could be safely managed non-operatively, colonic intussusception in adults require mandatory operative treatment because
many cases are associated with malignant bowel tumors [7,8].
Case presentation
Mr G.I.E, 86-years-old retired civil servant, presented via the
Accident and Emergency department of the hospital on referral
from a peripheral hospital in September 2023 with 5-days history of post-prandial central abdominal discomfort, abdominal
distension, poor appetite, inability to open his bowels properly
and occasional haematochezia. He had a single episode of vomiting at the onset and admitted to have lost some weight. He
was a known hypertensive and was regular with his medications. His past surgical history was unremarkable.
Clinically, he appeared frail and dehydrated. His vital signs
were unremarkable. The abdomen was distended, globally soft
and slightly tender, but not peritonitic. There was a palpable
mobile mass, the size of an avocado pear, situated at the right
upper abdominal region and partly extended into the right lower quadrant.
He came with an abdominal ultrasound scan report which
confirmed intussusception.
The abdominopelvic CT scan showed “the small bowel telescoping through the transverse colon up to the splenic flexure.
The intussusceptum measured 16.9 cm while the intususcipiens
measured 18.5 cm. There was associated dilated central bowel
loops with air-fluid levels”. The radiological conclusion was colocolonic intussusception involving the transverse colon.
From all the foregoing, our clinical diagnosis was incomplete
large bowel obstruction secondary to colonic intussusception.
His PCV was 28%, the serum potassium was 2.8 mmol/L but
the viral markers were negative for HIV and hepatitis B and C.
He was duly worked up for an exploratory laparotomy. The
patient received 1-unit of blood transfusion and correction of
hypokalaemia. He had urethral catheterization, bowel preparation and was commenced on total parenteral nutrition.
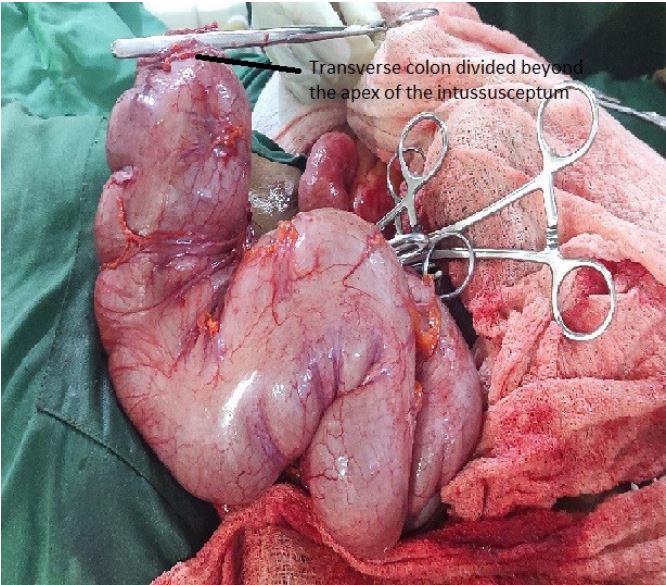
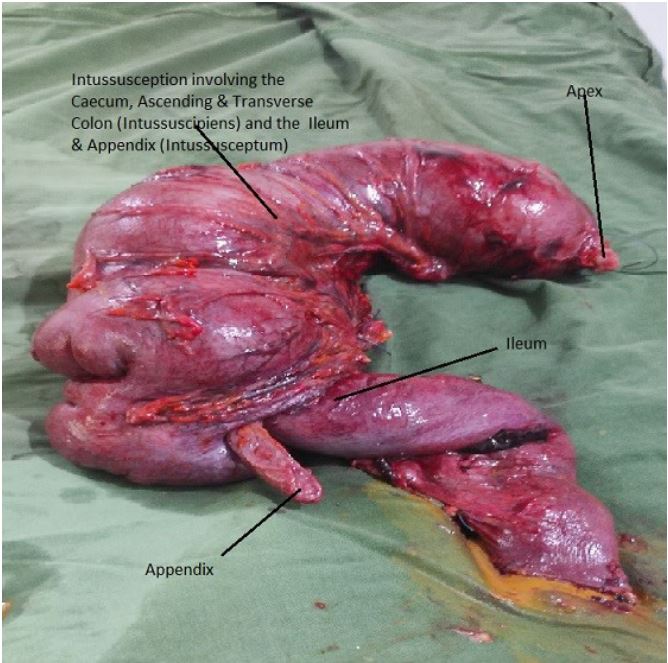
Intra-operatively, we found the invagination of the terminal
ileum, proximal part of the vermiform appendix and caecum
into the ascending and transverse colon. The intussusceptum
extended up to the splenic flexure (Figures 1-3). The right iliac
fossa was empty and there was 300 mls of serosanquinous fluid in the peritoneal cavity.
An extended right hemicolectomy was performed with primary ileo-colonic anastomosis. Anal dilation was done at the
conclusion of the operation.
The histology report revealed haemorrhagic necrosis with
marked mucosal fragmentation and vascular congestion in the
ileal section of the intussusceptum and colonic parts of the intususcipiens. No malignancy was identified.
The patient made an uneventful post-operative recovery and
was discharged home on the 8th day after surgery. He’s been followed up at the outpatient surgery clinic for 6-months and has
remained clinically well.
Discussion
Our patient presented in the 9th decade of life, an uncommon age for the development of intussusception. About 95% of
cases of this disease are seen in children below 16 years, with
the majority presenting during infancy [1].
The triad of colicky abdominal pain, presence of a palpable
abdominal lump and the passage of red currant jelly stool in a
child is pathognomonic of intussusception. This classical triad is
only present in about 2% of adults with the disease [9]. The patient presented in this report had a palpable lump and abdominal discomfort, but red currant jelly stool was absent. Rather,
the history of occasional haematochezia was obtained. These
clinical features mimicked the manifestation of intussusception
in children and therefore simplified the diagnosis of this disease
in our patient.
Where imaging investigations like abdominal ultrasound
scan and CT scan are available, the definitive diagnosis of adult
intussusception is straight forward, as in the case presented [6].
The definitive management of adult intussusception requires
mandatory surgical treatment because the majority is due to a
primary pathology, which may be bowel tumour [7]. When the
colon is involved in adult intussusception, malignancy must be
excluded [8]. Laparoscopic surgery where available, rather than
the open surgical approach, provides a minimally invasive and
preferred option for the management of intussusception particularly in the elderly adult patient [10]. Less blood loss, lower
morbidity and shorter time to recovery are some of the benefits
of the laparoscopic procedure. Our patient received the open
surgical operation because laparoscopic surgery was not available at our centre at the time of treatment.
Idiopathic intussusception, where no primary lesion is macroscopically and histologically identified as being the cause and
lead point of the disease, occurs mostly in children [2]. Curiously, our patient presented with this form of the disease in his
9th decade of life. The colonic site of involvement necessitated
resection of the intussusception by an extended right hemicolectomy in the case presented.
Conclusion
In conclusion, adult intussusception can present with clinical
features which are similar to those of the paediatric condition,
even in the 9th decade of life. The definitive diagnosis in such
cases is often straight forward, both clinically and radiologically.
However, surgical treatment is mandatory in adult colonic intussusception in order to exclude a possible neoplastic cause and
to treat any associated intestinal obstruction.
Declarations
Conflict of interest: None.
Funding: None.
Ethical approval: This case report is exempt from ethical approval in our institution.
References
- Russel RCG, Williams NS, Bulstrode CJK (Editors). Acute intussusception. In: Bailey and Love’s short practice of surgery. 23rd Edition. Arnold; London. 2000: 1067-69.
- Mbah N. Adult intussusception: Current perspective. Orient Journal of Surgical Sciences. 2021; 2: 1-13.
- Zubaidi A, Al-Saif F, Silverman R. Adult intussusception: A retrospective review. Dis. Colon Rectum. 2006; 49: 1546-51.
- Ugwu BT, Mbah N, Yiltok SJ, et al. Adult Intussusception: The Jos Experience. West African Journal of Medicine. 2001; 20: 213-216.
- Gordon RS, O’Dell KB, Namon AJ et al. Intussusception in adultsa rare disease. J Emerg Med. 1991; 9: 337-42.
- Valentini V, Buquicchio GL, Galluzo M, et al. Intussusception in adults: The role of MDCT in the identification of the site and cause of obstruction. Gastroenterology Research and Practice. 2016; 5623718. http://dx.doi.org/10.1155/2016/5623718
- Su T, He L, Zhou T, et al. Most adult intussusception are caused by tumours: A single-centre analysis. Cancer Management and Research. 2020; 12: 10011-15.
- Sanders GB, Hagan WH, Kinnaird DW. Adult intussusception and carcinoma of the colon. Ann Surg. 1958; 147: 796- 804.
- Onkendi EO, Grotz TE, Murray JA, et al. Adult intussusception in the last 25 years of modern imaging: Is surgery still indicated? J Gastrointest Surg. 2011; 15: 1699-1705.
- Kang S, Lee SI, Min BW, et al. A multicenter comparative study between laparoscopic and open surgery for intussusception in adults. Colorectal Dis. 2020.