Introduction
The oral cavity has been described as “the window of general health” [1]. The oral health adverse effects due to tobacco
including common diseases, and rare conditions have been reported in various authors like Reibel J, Dhami B in their article.
The city of Western part of Maharashtra, where transport
workers like bus conductors and drivers who work prolong
hours and constitute an essential part of urban informal sector,
where health is undervalued.
The socioeconomically factor, illiteracy, poverty, work stress
is a constant physical and psychological due to changing shift,
prolong working hours and lack of knowledge about hazards of
tobacco, which all leads to habits which are majority of being
tobacco use [2,3].
There are various studies in relation to oral health and tobacco, which was carried out in laborers, coal mine and seafarers, these all belong to low socioeconomic status, however
their results have been similar [4-6].
There are a total of 5309 combined bus conductors and drivers working in city of Western part of Maharashtra, the aim of
the study is to assess oral health status and tobacco related
habits, its types, duration, frequency, it’s a Cross-Sectional Analytical Study carried out to assess the oral health status and tobacco related habits, type of tobacco, its duration, frequency,
type of lesions seen in bus conductors and drivers due to tobacco habit
Material and methods
The present study was a Cross-Sectional Analytical Study assessing the oral health status and tobacco related habits, type
of tobacco, duration, frequency and oral lesions in bus conductors and drivers in a city of Western Maharashtra.
The Ethical clearance was obtained from the Institutional
Research Board (IRB) and Institutional Ethical Committee (IEC).
The other related permissions from the Chief Executive Officer
Public Transport Organization.
The study was conducted at all the 7 bus depots of a city in
Western part of Maharashtra. On extensive literature search,
limited literature was found on prevalence of dental disease
in public transport worker population. Hence, P=prevalence of
50% was taken since there was no study was conducted previously in this population of this area. The sample size was determined by using the Single Proportional formula, (n=[Zα/2]2 P (1-p)/d2
) at 95% confidence interval, where, Zα/2=1.96,
P = prevalence of 50% is taken since there is no similar study
in the area and d = 5% of marginal error was taken.
Using this calculation, a sample size of 384 was obtained
which was rounded off to 500 i.e. 500 Conductors and 500 Drivers making it a total of 1000 participants.
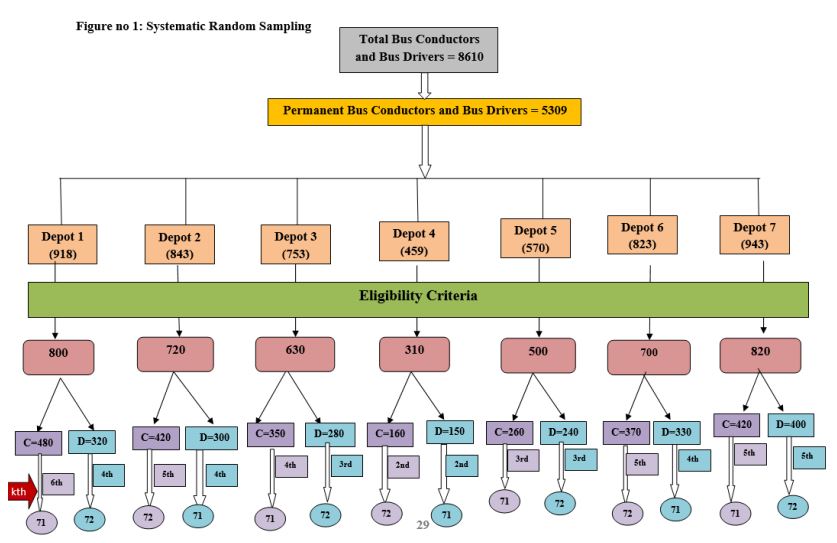
Systematic random sampling
The public transport organization in the city has a total of 7 bus depots accounting a total of 8610 bus conductors and drivers out of which 5309 were permanent.
A total of 500 Conductors and 500 Drivers were included in
the study. From the list obtained at the depots, every kth member was included in the study till a sample size of 71 conductors
and 72 drivers was obtained at each depot alternately. Thus,
making it a total sample size of 143 in each depot. The kth value
for each depot was different. This was done for uniform sampling at all the 7 bus depots.
The total permanent (bus conductors and drivers) in each
depot was 5309 as follows.
Table 1: List of total number of bus conductors and bus drivers
in each depot.
| Bus depots |
Total number of bus
conductors and drivers
|
| Depot 1 |
918 (376D+ 542C) |
| Depot 2 |
843 (317D+526C) |
| Depot 3 |
753 (252D+501C) |
| Depot 4 |
459 (243D+216C) |
| Depot 5 |
570 (248D+322C) |
| Depot 6 |
823 (285D+538C) |
| Depot 7 |
943 (383D+561C) |
| TOTAL |
5309 |
Inclusion criteria
Study participants who are willing to give voluntary written
informed consent, age group of 22-55 years with a minimum of
5 years’ service experience in the same occupation
Exclusion criteria
Study participants not willing to undergo examinations, who
had quit tobacco 1 yr ago were not included in the study.
Systematic random sampling
Was carried out in each depot and every ‘kth’ study participant was selected for the study in each depot. The ‘kth’ value
was different for bus conductors and bus drivers in each depot.
This was based upon the total number of bus conductors and
bus drivers in the respective depots.
The formula applied for systematic randomized sampling
was:
Total population of bus conductors / drivers in the respective
bus depot
k = After inclusion and exclusion criteria / Desired sample size of bus conductors/drivers
Where, k = interval at which bus conductor/bus driver were
selected.
The sampling technique is illustrated in the following figure 1.
Training and calibration of principal investigator
Training and calibration of the principal investigator was
done to overcome the difficulties in scoring the different levels
of diseases correctly. Intra-examiner calibration was undertaken by examining 30 individuals followed by their re-examination
a week later which resulted in 87% of diagnostic acceptability
with a kappa-value of 0.84.
Recording clerk and organizing clerk
Organising clerk duties were performed by the interns and
assistant provided by depot manager, however recording clerk
i.e. the intern who was also trained and calibrated and made
familiar with the preform in the Department of Public Health
prior to the conduction of the study.
Physical arrangements
Dental examination were conducted in the bus depots in a
mobile college dental van provided by the college administration.
Nature of information collected
The eligible and selected participants were approached as
follows:
Participant information and consent form: The participant
information sheet explaining the details of the study purpose
(Socio-demographic data, change in shift, details of tobacco
consumption, type, frequency, duration of consumption) and
procedure and informed consent in either English, Hindi or
Marathi language (as per convenience of the patient) was provided to the participants.
Data collection form and data collection procedure
The Oral Health Status of bus conductors and drivers were
recorded using WHO Oral Health Assessment Form 1997.
A Type-III clinical examination (American Dental Association
1970) was carried out using a mouth-mirror and a CPI probe
under good illumination carried out by the principal investigator. The examination was carried out in these depots till the
estimated sample size of 71 drivers and 72 conductors alternately were obtained from each depot. The study involved the
assessment of the bus conductors and drivers based on general
information, extra-oral examination, oral mucosal assessment
were recorded.
Method of data analysis
Following data collection, the responses were appropriately
coded, compiled systematically and entered into Microsoft Excel Spreadsheet (Version. 8.1). Statistical analysis was done using IBM Statistical Package for Social Sciences (SPSS) software
(Version 21.0. Armonk, NY: IBM Corp).
The p value less than 0.05 was considered statistically significant at confidence interval of 95%.
The following statistical tests were used for analysis of the
data:
Descriptive analysis
Unpaired t-test: It was used to compare the continuous variables between bus conductors and drivers.
Pearson’s correlation test: To assess the correlation between
Demographic status and oral health status and
Tobacco habits and oral health status.
Results
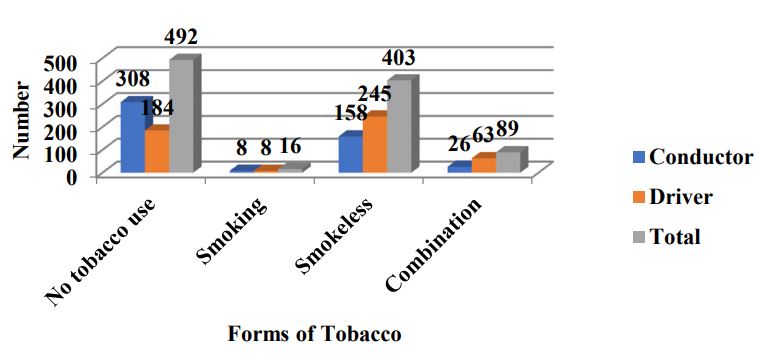
Out of total 1000 study participants, a majority were habitual to Smokeless tobacco form 403(40.3%) as compared to that
of Smoking 16(1.6%). This difference was statistically significant
(p<0.05). However, combined smokeless and smoking tobacco
was seen in 89 participants (8.9%).
Distribution of study participants based on type of tobacco:
(Table 2, Figure 2)
Out of total 500 bus conductors, 133(26.6%) had a habit
of chewing tobacco, whereas only 8(1.6%) smoke cigarettes.
Around 307 (61.4%) conductors were not using any form of tobacco.
Out of total 500 bus drivers, it was seen that 226(45.2%)
had a habit of chewing tobacco whereas 8(1.6%) smoke only
cigarettes. Around 185(37%) drivers were not using any form
of tobacco.
Table 2: Distribution of study participants based on form of To-
bacco use.
| Form of Tobacco |
Conductor N (%) |
Driver N (%) |
Total N (%) |
| No tobacco use |
308(61.6) |
184(36.8) |
492(49.2) |
| Smoking |
8(1.6) |
8(1.6) |
16(1.6) |
| Smokeless |
158(31.6) |
245(49) |
403(40.3) |
| Combination |
26(5.2) |
63(12.6) |
89(8.9) |
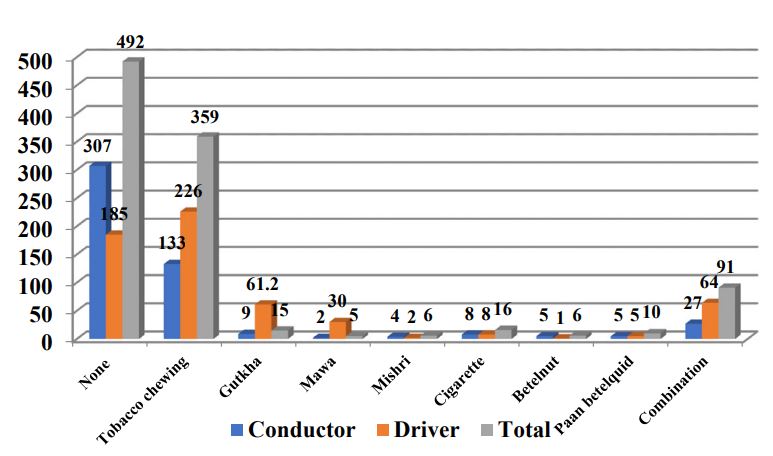
Table 3: Distribution of study participants according to tobacco
habits.
| Tobacco |
Conductor n (%) |
Driver n (%) |
Total N(%) |
| Type of tobacco use |
|
|
|
| None |
307(61.4) |
185(37) |
492(49.2) |
| Tobacco chewing |
133(26.6) |
226(45.2) |
359(35.9) |
| Gutkha |
9(1.8) |
6(1.2 |
15(1.5) |
| Mawa |
2(0.4) |
3(0.6) |
5(0.5) |
| Mishri |
4(0.8) |
2(0.4) |
6(0.6) |
| Cigarette |
8(1.6) |
8(1.6) |
16(1.6) |
| Betelnut |
5(1) |
1(0.2) |
6(0.6) |
| Paan betelquid |
5(1) |
5(1) |
10(1.0) |
| Combination |
27(5.4) |
64(12.8) |
91(9.1) |
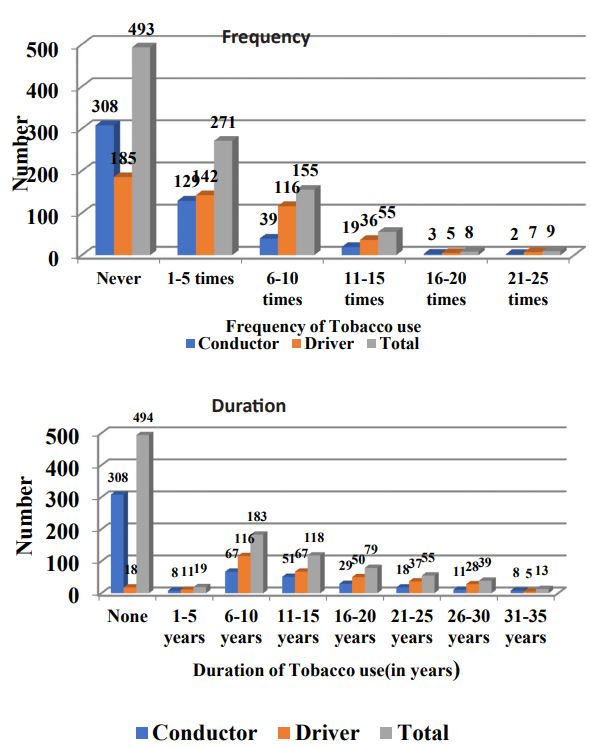
| Tobacco frequency |
|
|
|
| Never |
308(61.6 ) |
185(37) |
493(49.3) |
| 1-5 times |
129(25.8) |
142(28.4) |
271(27.1) |
| 6-10 times |
39(7.8) |
116(23.2) |
155(15.5) |
| 11-15 times |
19(3.8) |
36(7.2) |
55(5.5) |
| 16-20 times |
3(0.6) |
5(1) |
8(0.8) |
| 21-25 times |
2(0.4) |
7(1.4) |
9(0.9) |
|
Tobacco duration (in Years)
|
|
|
|
| None |
308(61.6) |
186(37.2) |
494(49.4) |
| 1-5 years |
8(1.6) |
11(2.2) |
19(1.9) |
| 6-10 years |
67(13.4) |
116(23.2) |
183(18.3) |
| 11-15 years |
51(10.2) |
67(13.4) |
118(11.8) |
| 16-20 years |
29(5.8) |
50(10) |
79(7.9) |
| 21-25 years |
18(3.6) |
37(7.4) |
55(5.5) |
| 26-30 years |
11(2.2) |
28(5.6) |
39(3.9) |
| 31-35 years |
8(1.6) |
5(1.0) |
13(1.3) |
Out of total 500 bus conductors and 500 bus drivers, it was
found that tobacco chewing habit was more likely seen in drivers 226(45.2%) as compared to that of conductors 133(26.6%).
Out of total 1000 study participants, around 359(35.9%)
were addicted to tobacco chewing habit, 16(1.6%) to cigarette
smoking and 91(9.1%) to a combination of both the habits. This
difference was statistically significant (p<0.05).
Out of total 1000 study participants around 492(49.2%) were
not using tobacco in any form.
The remaining 5.8% of the total study participants were using tobacco in other forms like Gutkha 15(1.5%), Mawa(0.5%),
Mishri (0.6%) and about 1.6% included the tobacco along with
Paan, betel nut and quid.
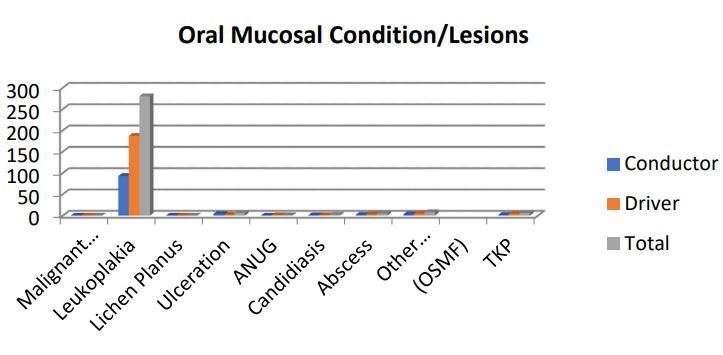
Table 4: Distribution of study participants based on presence
of oral mucosal lesions/conditions.
|
Oral mucosal
lesions/condition
|
Conductor N(%) |
Driver N(%) |
Total N(%) |
| Malignant Tumor |
0(0) |
0(0) |
0(0) |
| Leukoplakia |
93(18.6) |
187(37.4) |
280(28) |
| Lichen Planus |
0(0) |
0(0) |
0(0) |
| Ulceration |
4(0.8) |
2(0.4) |
6(0.6) |
| ANUG |
0(0) |
1(0.2) |
1(0.1) |
| Candidiasis |
1(0.2) |
1(0.2) |
2(0.2) |
| Abscess |
2(0.2) |
3(0.6) |
5(0.5) |
| Other Conditions (OSMF) |
3(0.6) |
5(1) |
80.8) |
| TKP |
2(0.4) |
4(0.8) |
6(0.6) |
| Not Recorded |
0(0) |
0(0) |
0(0) |
Distribution of study participants based on tobacco frequency and duration of tobacco use
Tobacco frequency: Out of total 500 bus conductors, around
129(25.8%) had a tobacco usage frequency of around 1 to 5
times a day and 22(4.4%) of using tobacco for more than 10
times a day. There were 2(0.4%) using tobacco for more than
20 times per day.
Out of total 500 bus drivers, around 142(28.4%) used tobacco for a frequency of 5 times per day whereas 41(8.2%) used
tobacco for more than 10 times a day. There were 7(1.4%) bus
drivers who used tobacco for more than 20 times.
Tobacco duration: Out of total 500 bus conductors, only
8(1.6%) used tobacco since 5 years whereas around 51(10.2%)
were using tobacco for 11-15 long years and 29(5.8%) had been
for a duration of long 20-30 years.
Out of total 500 bus drivers, 11(2.2%) used tobacco for a duration of 1-5 years whereas around 50(10%) used tobacco for a
duration of 20 years. Around 65(13%) had been using tobacco
for a duration of 20-30 years long.
Distribution of study participants based on presence of oral
mucosal lesions (Table 3, Figure 4)
Out of total 500 bus conductors, a majority 98(18.6%)
showed a presence of Leukoplakia, 3(0.6%) had Oral Submucous Fibrosis (OSMF). This difference was statistically significant
(p<0.05).
Out of total 500 bus drivers, a majority 187(37.4%) showed
a presence of Leukoplakia whereas 5(1%) had OSMF (Oral Submucous Fibrosis).
It was found that the Drivers as compared to Conductors
showed more number of Pre-cancerous lesions which was predominantly Leukoplakia followed by OSMF.
Out of total 1000 study participants, 280(28%) had Leukoplakia whereas 8(0.8%) had OSMF (Oral Submucous Fibrosis). This
difference was statistically significant (p<0.05).
Discussion
The study was conducted in all the bus depots of a city with
the objective to gather systematic information on oral health
status and tobacco habits in bus drivers and conductors in city
of western Maharashtra region. Assessing the impact of occupation on lifestyle. The oral health status was assessed using
WHO oral Health assessment form (1997)[32] and a general information sheet which the details of the study purpose (Sociodemographic data, change in shift, details of tobacco consumption, type, frequency and duration) was used.
It was seen in our study that almost 40.3% of the conductors
and drivers had the habit of Smokeless tobacco consumption
(i.e. Tobacco chewing, Gutkha, Mawa, Mishri, Paan with a mixture of betel nut, lime and tobacco). On the other hand, Cigarette smoking was seen less in comparison (1.6%) in this study
population as compared to smokeless form of tobacco. Similar
results were seen in the study done by Reddy et al. [7]. In the
group of transport workers in South India. The prevalence of
tobacco use was much higher in the present study conducted
in Maharsahtra as compared to that of the one conducted in
transport workers by Reddy et al.
In the present study, the tobacco usage was seen more in
bus drivers as compared to that of bus conductors which is in
consensus with results found in the study done by Reddy et al.
The reason probably could be that driers need more concentration, alertness and has more responsibility as compared to that
of conductors Gambhir in North India [8].
Different levels of Sociodemographic status are associated
with tobacco use in bus conductors and drivers. Among the
considered factors affecting the use of tobacco other than occupation, age and education have substantial effect on its usage.
They surely have an influence on tobacco usage. It was more
prevalent above the age 26 years.
Oral mucosal conditions and lesions could be due to infection (bacterial, viral, fungal), local trauma and or irritation (traumatic keratoses, fibroma, burns), systemic disease (metabolic or
immunological), or relate to lifestyle factors such as the usage
of tobacco, areca nut, betel quid, or alcohol. Important oral mucosal lesions were observed in the study which is in contradiction to study reports on an adult population [9-11]. Increase in
prevalence of oral mucosal lesions with age was reported in the
present study and in another study conducted elsewhere. The
most common oral mucosal lesion in the study was leukoplakia
which is in consensus with the studies [7,8]. Mandibular sulcus
region was the most common site of ulceration in this study and
in a an influence on tobacco usage. It was more prevalent above
the age 26 years.
Oral mucosal conditions and lesions could be due to infection (bacterial, viral, fungal), local trauma and or irritation (traumatic keratoses, fibroma, burns), systemic disease (metabolic
or immunological), or relate to lifestyle factors such as the usage of tobacco, areca nut, betel quid, or alcohol. Important oral
mucosal lesions were observed in the study which is in contradiction to study reports on an adult population [9-11]. Increase
in prevalence of oral mucosal lesions with age was reported in
the present study and in another study conducted elsewhere.
The most common oral mucosal lesion in the study was leukoplakia which is in consensus with the studies [7,8]. Mandibular
sulcus region was the most common site of ulceration in this
study and in another study conducted on workers engaged in
some other occupation [12,13]. This may be due to the habit of
keeping the tobacco quid most of the times in the mandibular
sulcus region. The tobacco frequency and duration was significantly associated with the oral mucosal lesions.
In the present study which was conducted in 1000 bus conductors and drivers of all 7 bus depots in a city, the bus conductors and drivers were made aware of their oral status and treatment needs. They were given the referral cards according to
their treatment needs. The participants were also provided the
oral health education along with the tobacco cessation counseling for the tobacco users and creating awareness of oral cancer
using posters, flipcharts and lectures.
Limitations of the study
In this cross sectional study we could not limit the Social
Desirability Bias where an individual gives a desired response,
which may have introduced while filling up the additional proforma. Also there was a possibility of occurrence of Hawthorne
effect while asking for deleterious habits.
Summary
The study sample of public transport workers i.e. bus conductors and bus drivers provided a unique opportunity to study
a population from diverse socioeconomic and geographic backgrounds. Hence, an attempt was made by taking up the study
to assess the oral health status and tobacco related habits, its
types, duration, frequency, in bus conductors and bus drivers
in all the bus depots of a city. The current study highlighted the
oral health status and tobacco habits its adverse effects on the
people of this specific population. It is the first study of its kind
as no other information is published regarding the oral health
status and tobacco habits of this specific population group in
this region and state.
Conclusion
The study concludes that occupational and environmental stress promoted the excessive use of smokeless tobacco
(40.3%) among the bus drivers and bus conductors all long day.
The prevalence of oral mucosal lesions was high amongst
the study population. The most common oral mucosal lesion
present was Leukoplakia (18.6%) followed by Oral Sub mucous
Fibrosis (OSMF) (0.6%) and most common location for the presence of oral mucosal lesions was buccal mucosa observed during study
There was a high prevalence of tobacco in this study population group which comprised of smoking, smokeless and a combination of both smoking and smokeless form of tobacco use.
Smokeless form of tobacco is more commonly used which is
40.3%. As reported by the study participants, deleterious habits
like tobacco started either for pleasure or peer influence but
with time it turned into a habit. Majority of the bus drivers and
also bus conductors reported their use in order to reduce tension, work pressure and maintain alertness.
References
- Choudhury AR, Ankola AV, Sankeshwari RM, Siddibhavi M, Vallakunja D, Khot AP, Deshpande A. Assessment of oral health status and tobacco-related habits among the employees of North-West Karnataka Road Transport Corporation (NWKRTC), Belagavi City-A Cross-Sectional Study. International Journal of Occupational Safety and Health. 2022 Sep 30; 12(4): 299-306.
- Sagtani RA, Thapa S, Sagtani A. Smoking, general and oral health related quality of life - a comparative study from Nepal. Health Qual Life Outcomes. 2020 Jul 31; 18(1):257.
- Singh SP, Misra SK, Chaudhary SS, Katyal R, Singh A, Joshi HS. Heath status of auto rickshaw drivers plying in Agra city. Med Pulse Int Med J. 2015; 2: 221–8
- Abbas I, Mohammad SA, Peddireddy PR, Mocherla M, Koppula YR, Avidapu R. Oral Health Status of Underground Coal Mine Workers of Ramakrishnapur, Adilabad District, Telangana, India - A Cross-Sectional Study. J Clin Diagn Res. 2016 Jan; 10(1): ZC28-31.
- Gambhir RS, Sogi GM, Veeresha KL, Sohi RK, Randhawa A, Kakar H. Dental health status and treatment needs of transport workers of a northern Indian city: A cross-sectional study. J Nat Sci Biol Med. 2013 Jul;4(2):451-6. 1. Park. 20th ed. New Delhi: Banarsidas Bhanot Publishers; 2009. Park’s textbook of Preventive and Social medicine.
- Rao BV, Suresh Babu AM, Kamalsha SK, Rao MS, Karthik K. Oral Health Status and Treatment Needs of Gunj Marketing Yard Laborers of Raichur City, Karnataka. J Pharm Bioallied Sci. 2017 JulSep;9(3):195-200.
- Reddyy CS and Reddy CVK.Oral health status and treatment needs of Karnataka State Road Transport Corporation Drivers and Employees in Mysore division.JIAPHD2016; 10(16): 221-27.
- Gambhir R, Sogi GM, Veeresha KL, Sohi RK, Randhawa A, Kakar H. Dental health status and treatment needs of transport workers of a northern Indian city: A cross-sectional study. Nat Sci Biol Med. 2013; 4(2): 451–6.
- Gordon M, Kusner W, Shifman A, Ronen E, Newbrun E. Assessing the dental treatment needs of an adult Israeli military population. Community Dent Oral Epidemiol. 1986; 14: 244–9.
- Pilot T, Lu ZY, Lin ZQ, Yen WP, Cao GR. Periodontal conditions in 35-44-year-old factory workers in Shanghai. Community Dent Oral Epidemiol 1989; 17: 216-19.
- Shizukuishi S, Hayashi N, Tamagawa H, Hanioka T, Maruyama S, Takeshita T, et al. Lifestyle and periodontal health status of Japanese factory workers. Ann Periodontol 1998; 3: 303–11.
- Reddy SS, Prashanth R, Devi Y, Chugh N, Kaur A, Thomas N.. Prevalence of oral mucosal lesions among chewing tobacco users: A cross-sectional study. Indian J Dent Res 2015; 26: 537-41.
- Sridharan G. Epidemiology, control and prevention of tobacco induced oral mucosal lesions in India. Indian J Cancer 2014; 51(1): 80-5.