Introduction
The impaction of mandibular third Molars (M3) affects a
significant portion of the European population, with a prevalence of 58% [1]. Surgical removal of the M3 ranks among the
most common procedures in oral surgery, due to factors such as
pericoronitis, caries, periodontitis, neoplastic changes, planned
orthognathic surgery, and resorption of the adjacent second
Molar (M2) [2].
To facilitate M3 extraction, bone removal is often necessary, depending on factors such as tooth position, angulation,
operator skill, and patient anatomy. However, this procedure
can leave a significant bony defect within the mandible, posing
a potential threat to the periodontal and bony support of the
second molar. Found that in 43.3% of cases [3], the Periodontal
Pocket Depth (PPD) at the distal portion of the M2 exceeded
7mm after M3 extraction. Subsequent research by [4] highlighted a 44.4% chance of Intrabony Defects (IBDs) greater than
4mm in individuals over 25 years old.
Early surgical intervention can prevent alveolar bone loss.
However, current UK NICE guidelines on wisdom teeth removal
adopt a reactive approach, aiming to reduce referrals for asymptomatic impacted wisdom teeth due to funding constraints
[5]. This strategy, though seemingly logical, may lead to compromised M2 conditions, yet the financial implications remain
unquantified.
Addressing complications associated with M2 post-M3 extraction, studies advocate for using patient-derived bone substitutes, emphasizing the superiority of autogenous grafts over
animal or synthetic sources [6]. Despite the disadvantage of
requiring a second procedure, autogenous bone grafts, commonly harvested from the mandible or iliac crest, have been a
conventional choice. The focus has recently shifted to dentine
due to its molecular properties resembling bone, particularly its
organic component consisting of 90% type I collagen and noncollagen proteins stimulating mesenchymal stem cells [7].
The Autogenous Dentine Graft (ADG) utilises the recently
extracted tooth, eliminating the need for a second procedure.
However, its efficacy is limited by the condition of the extracted
tooth [8]. Cost-effective and less technique-sensitive, dentine
grafts could be applied in both primary and secondary care,
potentially reducing post-operative complications for both patients and healthcare providers.
This review aims to assess current literature to answer the
research question: Can the periodontal health of a second molar be improved by placing an autogenous dentine graft following the surgical removal of a wisdom tooth? By addressing this
question, the review seeks to contribute valuable insights to future guidelines on mandibular third molar extractions.
Material and methods
The methodology of this review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, as outlined by [9].
To structure the review, a protocol employing the PICO system was devised to address the research question: Can the
periodontal health of a second molar be improved following the surgical removal of a wisdom tooth by the placement of an
autogenous dentine graft?
Population (P): Individuals requiring the surgical removal of
third molars
Intervention (I): Placement of an Autogenous Dentine Graft
(ADG)
Comparison (C): Conventional healing
Outcome (O): Periodontal Probing Depths (PPD) distal of the
second molar and the capacity of ADG to stimulate bone formation
To identify relevant literature, an electronic search was conducted using the keywords “Autogenous Dentine Graft”. The
search was limited to the dentistry category, and four key databases, namely MEDLINE, Dentistry & Oral Sciences, Academic
Search Complete, and Cumulative Index of Nursing & Allied
Health Literature (CINAHL) Ultimate, were selected through the
EBSCO platform.
The research question was deconstructed into five concepts:
Mandible, Third molar, Extraction, Dentine graft, and Periodontal. These concepts were linked using Boolean operators, and
wildcards were employed for variations in spelling and word
truncations.
The literature search included publications in the English
language from the last 5 years, encompassing randomized/
non-randomized control trials, cohort studies, and case-control
studies, aligning with the top half of the evidence pyramid hierarchy [10].
Inclusion criteria encompassed studies where ADG was
chair-side produced, uncontaminated bone substitution material, and reported outcomes at least 6 months postoperatively.
Exclusion criteria comprised studies involving wisdom teeth
removal for tumour resection, use of allogeneic or synthetic
grafts, absence of radiological or periodontal findings, and articles with vague or unclear design/methodology.
Outcome variables were defined as Periodontal Probing Depth (PPD) and bone height measured from the cement
enamel junction of the second molar. Research titles underwent screening, and abstracts were analysed for patient population and study characteristics, leading to the identification of
4 relevant papers.
Data extraction involved gathering general information,
eligibility, population and setting, method, participant characteristics, surgical method, intervention characteristics, control
measures, outcome measurement, results, and study quality. A
meta-analysis was precluded due to heterogeneous data, small
sample sizes, and variations in radiological imaging among studies.
To assess bias, the revised Cochrane risk-of-bias tool for
randomised trials (RoB 2) was applied, categorizing studies
into “low risk of bias,” “some concerns,” or “high risk of bias”
across five domains. Additionally, the 2011 Oxford Centre for
Evidence-Based Medicine (OCEBM) table was utilized to rank
literature by study design.
Mean and Standard Deviation (SD) figures from all studies
were compiled in a database. For studies lacking SD, the formula (SE=SD/√n) was applied, where n represents the sample
size. When studies measured bone height from multiple points,
the data was amalgamated into a single mean, allowing the calculation of a pooled SD using Cohen’s formula. Raw data from
studies presenting only means were calculated for both mean
and SD and are presented in this review.
Results
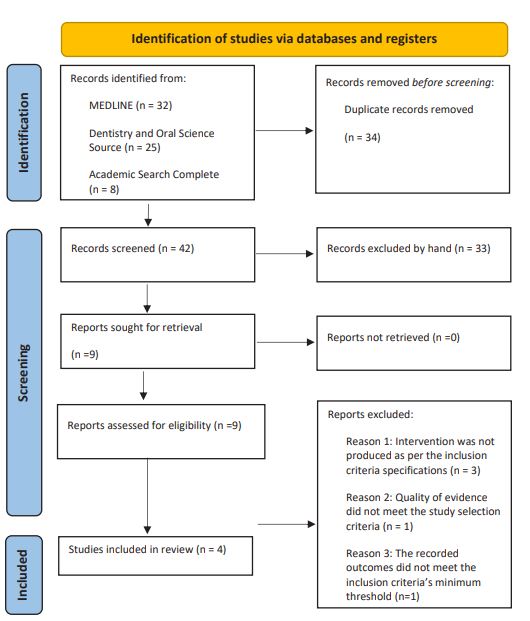
A comprehensive search across four databases - MEDLINE
(32 titles), Dentistry & Oral Sciences (25 titles), Academic Search
Complete (8 titles), and CINAHL Ultimate (11 titles) - yielded a
total of 76 titles. Following the elimination of duplicates, 42
unique records underwent screening of titles and abstracts.
This screening resulted in the removal of 33 papers, leaving
nine papers identified for full retrieval and examination.
Upon thorough examination, five manuscripts failed to meet
the selection criteria, resulting in a final inclusion of four papers
for this review. The entire search process and outcomes are visually presented in the flow chart depicted in Figure 1. This systematic approach ensures a robust selection of literature aligning with the review’s objectives.
A total of four articles were included in this review, exclusively comprising randomized control trials. The selected studies uniformly adopted a split-mouth design, wherein both
lower wisdom teeth necessitated extraction. One socket was
designated for the intervention, while the other served as the
comparison or control. Notably, [11] introduced an additional
dimension to their study by incorporating two patients requiring the removal of only one wisdom tooth, thereby diversifying
the demographic pool.
Table 1: Summary of four articles reviewed.
| Author |
Year |
Study
design |
OCEBM level of
evidence
|
No. of
participants
|
No. of
extractions |
Split mouth /
unilateral
|
Manufacture of tooth grinder
|
| Kuperschlag et al. [11] |
2020 |
RCT |
2 |
13 |
24 |
Both |
- |
| Mazzucchi et al. [12] |
2022 |
RCT |
2 |
10 |
20 |
Split mouth |
Smart Dentin Grinder™ |
| Sánchez et al. |
2020 |
RCT |
2 |
15 |
30 |
Split mouth |
Smart Dentin Grinder™ |
| Wushou et al. [13] |
2022 |
RCT |
3 |
5 |
10 |
Split mouth |
BonMaker® |
| Total |
|
|
|
43 |
84 |
|
|
| Mean |
|
|
|
10.75 |
21 |
|
|
All the studies incorporated a full thickness flap design for
their surgical access, ensuring a standardized approach across
the board. Noteworthy differences emerged in the size of particulate materials used, with studies employing the Smart Dentin Grinder generally yielding smaller particles compared to
those using the BonMaker.
Table 2:Summary of surgical considerations.
| Author |
Presurgical rinse |
Mucoperiosteal flap
design
|
Size of particulate |
Additional materials
used
|
Antibiotics |
|
Kuperschlag et al 2020 [11]
|
Yes – 0.2%
Chlorohexidine
|
Full thickness -Triangular
|
|
Yes - gelatine sponge |
Antibiotics given
amoxicillin for 5 days
|
|
Mazzucchi et al 2022 [12]
|
No |
Full thickness -Triangular
|
300 –1200 μm |
No |
Antibiotics given
co-amoxiclav for 6 days
|
| Sánchez et al 2020 |
No |
Full thickness - Envelope
|
300 –1200 μm |
Yes - gelatine sponge |
Antibiotics not routinely
given
|
| Wushou et al 2022 [13] |
No |
Full thickness -Triangular
|
425 –1500 μm |
Rubber drainage strip |
Antibiotics given |
Table 3: Measurement of Outcomes and Duration of Each Trial.
| Author |
Kuperschlag et al. [11] |
Mazzucchi et al. [12] |
Sánchez et al. |
Wushou et al. [13] |
| Start date |
- |
- |
September 2018 |
May 2021 |
| End date |
- |
- |
September 2019 |
- |
|
Duration of participation
|
12 months |
6 months |
6 Months |
6 months |
Periodontal pocketing of
the
lower 2nd molar
|
Probing depths taken
pre-op,
3 and 12 months
after
surgery and mea-
sured
in millimetres.
|
Probing depths taken pre-op,
3 and 6
months after
surgery and measured
in
millimetres.
Measurements
taken from three
pocket
locations: Disto-buccal,
Mid-
distal,
Disto-lingual
|
Probing depths taken pre-op,
3
and 6 months after
surgery and
measured in
millimetres.
Measurements
taken from three
pocket
locations: Disto-buccal,
Mid-distal,
Disto-lingual
|
Probing depths taken pre-op
and
6 months after
surgery and mea-
sured
in millimetres.
|
Radiographic interpreta-
tions
|
Pre op OPG
12 months
Post op OPG
Bone loss
in millimetres.
|
Pre op PA
6 Month post
op PA
Bone loss in
millimetres.
Measurement
from CEJ to the bone
peak
|
Cone beam computed
tomogra-
phy used at 6
months to compare
both
sites.
Measurement from
IAN to bone
crest.
|
Pre and post op OPG |
Table 4: Risk of Bias Tool Version 2 for Periodontal Probing Depth
|
D1 |
D2 |
D3 |
D4 |
D5 |
Overall |
|
Kuperschlag et al 2020 [11]
|
 |
 |
|
|
|
|
|
Mazzucchi et al 2022 [12]
|
|
|
|
|
|
|
| Sánchez et al 2020 |
|
|
|
|
|
|
| Wushou et al 2022 [13] |
|
|
 |
|
|
|
|
low risk
|
Some
concerns
|
High risk
|
Table 5: Picture summary of risk of bias tool version 2 for bone height.
|
D1 |
D2 |
D3 |
D4 |
D5 |
Overall |
|
Kuperschlag et al 2020 [11]
|
|
|
|
|
|
|
|
Mazzucchi et al 2022 [12]
|
|
|
|
|
|
|
| Sánchez et al 2020 |
|
|
|
|
|
|
| Wushou et al 2022 [13] |
|
|
|
|
|
|
|
low risk
|
Some
concerns
|
High risk
|
Table 6: Bar Graph of Risk of Bias Tool Version 2 for all Assessed Outcomes.
In terms of postoperative care, all reviewed trials routinely
administered antibiotics after the extraction, except for the
study conducted by Sánchez et al. This practice contrasts with
the current guidelines of the National Institute for Health and
Care Excellence (NICE) in the UK, which advises against routine
antibiotic use post-extraction. The existing evidence suggests
that such a regimen has minimal impact on bone remodelling
and may pose a greater risk of adverse reactions, such as anaphylaxis [14].
One notable departure from the common practice was observed in the study by Kuperschlag et al (2020) [11], where a
chlorhexidine mouth rinse was administered before surgery.
While there is some evidence supporting its potential to reduce
the occurrence of alveolar osteitis, its efficacy in promoting
bone healing remains inconclusive [15].
For a comprehensive overview of the surgical specifications
of each study, refer to Table 2, while Table 3 provides details
regarding the duration of the procedures and the assessment of
outcomes. These nuanced variations in procedural approaches
underscore the importance of understanding the diverse methodologies employed across the studies included in this review.
Table 7: Periodontal probing depth results summary.
|
Kuperschlag et al 2020 [11]
|
Mazzucchi et al 2022 [12]
|
Sánchez et al 2020
|
Wushou wt al 2022 [13]
|
|
Control |
Test |
Control |
Test |
Control |
Test |
Control |
Test |
| Pre surgery mean (SD) |
- |
- |
4.60mm (1.67) |
4.53mm (1.13) |
5.92mm |
5.97mm |
3.50mm |
3.16mm |
| 3 month mean (SD) |
4.00mm (0.853) |
1.31mm (0.751) |
4.20mm (1.03) |
3.06mm (1.08) |
6.00mm |
4.12mm |
- |
- |
| 6 month mean (SD) |
- |
- |
3.76mm |
(1.04) |
3.16mm (0.98) 5.68mm |
4.10mm |
- |
- |
| 12 month mean (SD) |
4.45mm (0.954) |
1.15mm (0.801) |
- |
- |
- |
- |
- |
|
|
Statistical significance
|
Yes: P<0.001
|
No:
Pre surgery
P=0.368
6 months
P=0.065
Yes:
3
months P<0.033
|
Yes:
P=0.038
|
- |
Table 8: Radiographic results for bone height.
|
Kuperschlag et al 2020 [11]
|
Mazzucchi et al 2022 [12]
|
Sánchez et al 2020
|
Wushou wt al 2022 [13]
|
|
Control |
Test |
Control |
Test |
Control |
Test |
Control |
Test |
| Pre surgery mean (SD) |
- |
- |
-2.09mm (0.43) |
-2.03mm (0.56) |
- |
- |
- |
- |
| 6 months mean (SD) |
- |
- |
-0.96mm (0.33) |
-0.62mm (0.58) |
- |
- |
- |
- |
| 12 months mean (SD) |
-4.20mm
(1.2) |
-1.05mm
(0.91) |
- |
- |
- |
- |
- |
- |
| Bone gain |
- |
- |
1.13mm (0.41) |
1.41mm (0.87) |
-0.68mm |
0.54mm |
- |
- |
|
Bone density at 6 months
|
- |
- |
- |
- |
1122.26 HU |
1538.93 HU |
- |
- |
|
Statistical significance
|
Yes:
P<0.001
|
No:
Pre surgery
P=0.368
6 months
P=0.065
Yes:
3
months P<0.033
|
Yes:
P=0.038
|
- |
To ensure a comprehensive assessment of potential bias, the
second iteration of the ‘Risk of Bias’ tool from the Cochrane Collaboration was employed to scrutinize all four papers, focusing
on both reviewed outcomes.
This assessment considers five key domains:
Domain 1. Randomisation process
Domain 2. Deviations from the intended interventions
Domain 3. Missing outcome data
Domain 4. Measurement of the outcome
Domain 5. Selection of the reported result
Regarding the evaluation of bias in measuring the periodontal probing depth outcome, the results varied across the studies. Two studies were classified as having a ‘low risk’ of bias, one
displayed ‘some concerns,’ and one was deemed ‘high risk,’ as
delineated in Table 4.
Specifically, Mazzucchi et al (2022) [12] and Sánchez et al
(2020) exhibited a ‘low risk’ across all domains, indicating a robust methodological approach. Conversely, Wushou et al demonstrated ‘some concerns’ or ‘high risk’ in all domains, signifying
potential limitations in the study design and implementation.
These insights into bias considerations enhance the interpretability of the findings and reinforce the importance of critically
appraising the methodological quality of the included studies.
To comprehensively evaluate potential bias in the assessment of bone height distal to the second molar, the Cochrane
‘Risk of Bias’ tool was applied. The findings are summarized in
Table 5 and provide insights into the methodological robustness
of the included studies. The assessment encompasses the same
five domains as mentioned earlier.
Among the studies reviewed, one was classified as having a
‘low risk’ of bias, two exhibited ‘some concerns,’ and one was
categorized as ‘high risk.’ Notably, Sánchez et al (2020) emerged
as the sole study demonstrating ‘low risk’ across all domains, indicating a robust methodological approach. Conversely, Wushou et al (2022) [13] exhibited concerns or ‘high risk’ in all domains, suggesting potential limitations in the study design and
execution. These insights into bias considerations add depth to
the interpretation of outcomes, emphasizing the importance of
critically appraising the methodological quality of studies assessing bone height distal to the second molar.
The studies reviewed had an overall low risk in 50% of the
domains. In the domain of missing outcome and measurement
of the outcome, 37.5% of the papers reviewed were of high risk.
A summary of all domains is portrayed in table 6.
All included studies employed a split-mouth design, where
each patient received both the interventional and control treatments through the extraction of lower left and right third molars. This methodological approach, while acknowledging the
inherent variability in each extraction, effectively controlled
external and internal environmental factors that could potentially influence the results. Despite the individualized nature of
each extraction, this design enhances the internal validity of the
studies.
Limited evidence in this field can be attributed to the recent
development of Autogenous Dentine Graft (ADG) techniques.
Consequently, high-quality evidence in the form of robust studies is constrained. This limitation underscores the need for cautious interpretation of positive results, urging clinicians to await
larger trials before considering the widespread adoption of
tooth grinding machines in their practices.
Across all four studies, a consensus emerged that periodontal probing depths were reduced when ADG was employed.
However, the magnitude of the difference between the test and
control groups varied significantly between studies. Notably,
Kuperschlag et al (2020) [11] achieved the most pronounced
intervention success, with periodontal pockets differing by an
average of 3.3mm between the two groups at the one-year review. In contrast, Mazzucchi et al (2022) [12] reported positive
results, but the difference was only 0.6mm after 6 months. A
statistical analysis by Mazzucchi et al revealed significance only
at the 3-month review, unlike the other studies, which identified a statistically significant difference in favour of ADG in every
review period.
Table 7 provides a comprehensive summary of the results
for all studies, depicting the periodontal probing depths of the
second molar. The mean periodontal probing depth distal to
the M2 was 2.83mm when using ADG compared to 4.7mm at
the control site, indicating a 66% reduction in the periodontal
pocket on average at the 3-month review.
Between 6 to 12 months, the control site exhibited an average reduction of 0.07mm, while the intervention site saw a
further reduction of 0.03mm in the periodontal pocket. This
suggests that most of the healing occurs within the initial three
months for both ADG and control sites. These nuanced findings
contribute valuable insights into the temporal dynamics of periodontal healing post-ADG intervention.
Across all four studies, both Autogenous Dentine Graft (ADG)
and conventional healing were associated with an increase in
bone height. However, the gain in bone height was consistently
greater in sites treated with ADG. Statistical significance in favour of the intervention was observed in two papers, while the
other two suggested that ADG might be beneficial for bone formation.
The combined mean results revealed a positive gain of
0.9mm of bone in sites treated with ADG up to 12 months,
whereas sites undergoing conventional healing experienced a
subsequent loss of 1.25mm of bone. This significant difference
of 2.15mm corresponds to an additional 16% of bony coverage
when utilizing ADG, relative to the average length of a distal
root of the second molar (13.35mm).
Sánchez et al (2020) and Mazzucchi et al (2022) [12] reported a positive crestal bone height gain exceeding 0mm. This
suggests that the removal of the wisdom tooth improved bone
height to a level superior to that before the surgery. This observation can be attributed to the common mesial or horizontal
impaction of wisdom teeth, potentially influencing pre-surgery
bone height, as bone does not adhere to enamel surfaces of a
crown.
While bone density data was recorded in only one study,
it yielded a statistically significant result (P<0.001). The Hounsfield (HU) range for average bone density typically varies between 300 to 3000 [16]. As detailed in Table 8, Sánchez et al
(2020) reported a notable 37% increase in bone density when
using ADG, compared to conventional healing, at the 6-month review. This finding provides valuable insights into the potential
benefits of ADG in enhancing bone density, complementing the
radiographic evidence of increased bone height.
Discussion
This systematic review critically evaluated the efficacy of
Autogenous Dentine Grafts (ADG) in promoting bone regeneration following the extraction of mandibular third molars (M3).
Traditionally, extracted teeth were regarded as biomedical byproducts and often discarded as clinical waste. However, advancing insights into bone remodelling have led to the recognition of extracted teeth as potential sources for generating bone.
Notably, bone mineral density is crucial for periodontal health,
suggesting a potential connection between bone and periodontium health. The American Association of Oral and Maxillofacial
Surgeons recommends bone grafts for patients at an increased
risk of osseous defects post-extraction. In contrast, current
UK guidelines lack explicit recommendations for graft placement following M3 extraction, possibly due to historical cost
constraints associated with synthetic or animal-derived grafts.
Further research may position ADG as a routine post-extraction
step, addressing postoperative periodontal complications and
future-proofing bone for potential implant procedures.
Traditional autogenous grafts sourced from the patient typically involve a second procedure or an extended post-operative
healing process. Utilizing components from extracted teeth circumvents the need for a second procedure and proves to be
cost-effective compared to alternative grafts.
The positive outcomes observed across all reviewed articles
align with the theme of ADG demonstrating efficacy in both observed outcomes. The limited evidence available raises the possibility of publication bias, where studies indicating detrimental
effects of the intervention may not be publicized, potentially
influenced by manufacturers of tooth grinding machines.
Notably, power calculations were lacking in most studies, except in Sánchez et al (2020), who recommended a minimum
of 10 patients for both the intervention and control groups to
generate statistically relevant evidence. The absence of power
calculations increases the risk of type I and type II errors within
a study. Nevertheless, three out of four studies in this review
adhered to Sánchez et al's proposed number of patients.
Given that significant bone dimensional changes occur within the first three months post-standard extraction, extending
the observation period to a minimum of 12 months in future
studies would provide a more comprehensive understanding of
the long-term effects of ADG on bone remodelling.
The split-mouth design employed in the reviewed studies,
while minimizing external factors affecting results, revealed individual variations in tooth characteristics. While three articles
assessed the difficulty of wisdom tooth extraction, they did not
explore how surgical bone removal might impact the body's
ability to undergo osteogenesis in severe bone defects. Random assignment of the intervention may have mitigated this
confounding factor, but the importance of bone regeneration
in severe defects was not emphasized in the reviewed papers.
Combining results demonstrated a mean periodontal probing depth distal to the second molar of 2.83mm with ADG, indicating healthy periodontal tissue per British Society of Periodontology standards. In contrast, the control group exhibited
mean periodontal probing depths exceeding 4.7mm, indicative
of a compromised periodontium requiring professional intervention. The nearly 2mm average difference equates to a remarkable 66% improvement in periodontal pocket depth with
ADG.
Additionally, the combined evidence suggested a positive
gain of 0.9mm of bone within the osseous defect with ADG,
compared to a negative loss of 1.25mm at the control site. This
indicates that ADG enhanced the area beyond its pre-surgery
state. The 2.15mm average difference, corresponding to 16%
of the distal root surface of the second molar, could potentially
impact the staging and grading of a patient's periodontal condition according to the British Society of Periodontology classification system. This potential reclassification may offer the
opportunity for more effective hygienic therapy.
Dental Cone Beam Computer Tomography (CBCT) was underutilized in the literature, with most studies relying on twodimensional methods. Future trials assessing ADG could benefit from three-dimensional analysis to ensure more accurate
recording of bone formation and minimize measurement bias.
Considering the potential influence of ethnicity on bone
structure and density, the lack of participant ethnicity data in
the reviewed studies raises concerns about limited representation and potential statistical distortions. Additionally, the geographic bias in publications, predominantly from Europe, may
further impact the generalizability of results.
Given the nature of the intervention, ensuring both patients
and researchers remain unaware of the treated socket presents challenges. The additional time required for ADG procedures
may influence patient confidence in identifying the treated
socket, potentially introducing the Hawthorne effect where patient behaviour changes due to observation, impacting the success or failure of the intervention.
As consumer awareness grows, the origin and development
of materials used in medical procedures, including dentistry,
become significant considerations for patients. ADG offers an
alternative to allografts and xenografts, avoiding foreign body
interactions and poor biocompatibility associated with certain
bone substitutes. The historical use of bovine bone substitutes
like Bio-Oss highlighted issues of poor integration and disrupted healing, emphasizing the potential advantages of ADG in
augmenting osseous defects, protecting soft bone, and aiding
wound healing without compromising patients or practitioners
financially.
Conclusion
Autogenous dentine grafts emerge as a potential solution
in scenarios where the periodontal health of the second molar
(M2) is at risk following the surgical extraction of the mandibular third molar (M3). High-risk cases, such as severely impacted
M3s or instances requiring excessive bone removal, may particularly benefit from ADG. While early studies on ADG show
promise, the current limitations in available evidence warrant
further research with larger participant cohorts to establish the
justification for integrating ADG into primary care settings.
Given the existing constraints, future studies should extend
their observations over a standard bone remodeling timespan,
ideally 12 months, to ensure a more comprehensive understanding of the long-term effects of ADG. Additionally, the potential for increased measurement accuracy of bone gain could
be realized by employing Cone Beam Computed Tomography
(CBCT) over traditional two-dimensional imagery. This technological advancement could enhance the precision of assessing
bone regeneration and contribute to the overall reliability of
study findings.
In conclusion, while the initial findings are encouraging, the
application of autogenous dentine grafts in routine clinical practice requires further substantiation through extensive research
and a meticulous evaluation of long-term outcomes.
References
- Carter K, Worthington S. Predictors of third molar impaction: a systematic review and meta-analysis. Journal of dental research. 2016; 95(3): 267-276.
- Passarelli PC, Pasquantonio G, D’Addona A. Management of surgical third lower molar extraction and postoperative progress in patients with factor VII deficiency: A clinical protocol and focus on this rare pathologic entity. Journal of Oral and Maxillofacial Surgery. 2017; 75(10): 2070-e1.
- Kugelberg CF, Ahlströ U, Ericson S, Hugoson A. Periodontal healing after impacted lower third molar surgery: a retrospective study. International journal of oral surgery. 1985; 14(1): 29-40.
- Kugelberg CF. Periodontal healing two and four years after impacted lower third molar surgery: A comparative retrospective study. International journal of oral and maxillofacial surgery. 1990; 19(6): 341-345.
- Gadiwalla Y, Moore R, Palmer N, Renton T. Where is the ‘wisdom’in wisdom tooth surgery? A review of national and international third molar surgery guidelines. International Journal of Oral and Maxillofacial Surgery. 2021; 50(5): 691-698.
- Serafini G, Lollobrigida M, Fortunato L, Mazzucchi G, Lamazza L, et al. Postextractive alveolar ridge preservation using L-PRF: Clinical and histological evaluation. Case reports in dentistry. 2020.
- Sampath TK, Reddi AH. Discovery of bone morphogenetic proteins–A historical perspective. Bone. 2020; 140: 115548.
- Gual-Vaqués P, Polis-Yanes C, Estrugo-Devesa A, Ayuso-Montero R, Marí-Roig A, et al. Autogenous teeth used for bone grafting: A systematic review. Medicina oral, patologia oral y cirugia buccal. 2018; 23(1): e112.
- Page, M.J, Moher, D, Bossuyt, P.M, Boutron, I, Hoffmann, T.C, Mulrow, C.D, Shamseer, L, Tetzlaff, J.M, Akl, E.A, Brennan, S.E. and Chou, R, (2021). PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. bmj, 372.
- Trombelli, L, Farina, R, Marzola, A, Bozzi, L, Liljenberg, B. and Lindhe, J, (2008). Modeling and remodeling of human extraction sockets. Journal of clinical periodontology. 2008; 35(7): pp.630-639.
- Kuperschlag A, Keršytė G, Kurtzman GM, Horowitz RA. Autogenous Dentin Grafting of Osseous Defects Distal to Mandibular Second Molars After Extraction of Impacted Third Molars. Compendium of Continuing Education in Dentistry (Jamesburg, NJ: 1995). 2020; 41(2): 76-82.
- Mazzucchi G, Lollobrigida M, Lamazza L, Serafini G, Di Nardo D, et al. Autologous Dentin Graft after Impacted Mandibular Third Molar Extraction to Prevent Periodontal Pocket Formation-A Split-Mouth Pilot Study. Materials. 2022; 15(4): 1431.
- Wushou A, Zheng Y, Han Y, Yang ZC, Han FK. The use of autogenous tooth bone graft powder in the treatment of osseous defects after impacted mandibular third molar extraction: a prospective split-mouth clinical pilot study. BMC Oral Health. 2022; 22(1): 1-6.
- Lodi G, Azzi L, Varoni EM, Pentenero M, Del Fabbro M, et al. Antibiotics to prevent complications following tooth extractions. Cochrane Database of Systematic Reviews. 2021; 2.
- Brunello G, Becker K, Scotti L, Drescher D, Becker J, et al. The effects of three chlorhexidine-based mouthwashes on human osteoblast-like SaOS-2 cells. An in vitro study. International Journal of Molecular Sciences. 2021; 22(18): 9986.
- Kim KJ, Kim DH, Lee JI, Choi BK, Han IH, et al. Hounsfield units on lumbar computed tomography for predicting regional bone mineral density. Open medicine. 2019; 14(1): 545-551.