Introduction
In this revision, we will try to address the entrapment neuropathies of the median nerve, from a clinical and practical approach, so as the family physicians or non-specialist practitioners can know more about these pathologies. Despite Carpal
Tunnel Syndrome (CTS) is by far the most common entrapment
neuropathy, we should know that not all the pains or paresthesias in the volar side of the hand or forearm are due to CTS. We
will deliberately avoid too many anatomic data or specific treatment details, of limited utility in general practice. Nevertheless,
in the references the reader can get much more information. If
this paper can clarify several questions regarding the median
nerve compression, signs and symptoms, the authors will feel
more than happy, as this is our main objective.
Entrapment neuropathies: Usually, peripheral nerves are
prone to entrapment when the pass-through areas of fibrous
or fibro osseous tunnels. Other factors can influence nerve entrapment at different locations, like local or generalized oedema
(tenosynovitis, arthritis, hormonal changes.), space occupying
lesions (tumors, hematoma…), accumulation of substances
(amyloidosis, mucopolysaccharidosi). Entrapment Neuropathies (EN) are heterogenous conditions due to different underlying pathophysiology, thus producing very different signs and
symptoms, depending upon the nerve, level of compression
and other causes. The pathophysiology of the compression will
give us the clue for the diagnosis and treatment. The definition
of EN is varied. A good definition could be: “disorders of the
peripheral nerves that are characterized by pain and/or loss of
function (sensory and/or motor) as a result of chronic compression of the nerves” [1]. The main objective of this paper is to
draw a schematic map to distinguish among these three different places of compression of the Median Nerve (MN) so as not
to mistake them. This knowledge is the only way for an early
diagnosis, that is always based upon a clinical suspicion. This
is crucial because precocious nerve injuries may be reversible,
while prolonged ones may be not. This is applicable not only for
family physicians/general practitioners but also for specialists.
The median nerve: The MN is a mixed, sensory and motor
nerve, innervating areas of the forearm and hand. It travels
down the front of the upper arm, across the front of the elbow
into the forearm. There it innervates the flexor and pronator
muscles. It also supplies innervation to the thenar muscles and
lateral two lumbricals in the hand. This is regarding its motor
function. The MN travels through the mid forearm (as its name,
“median”), into the hand through the carpal tunnel, giving sensory function to the palm, more precisely to the thumb, finger,
middle and radial side of the ring finger.
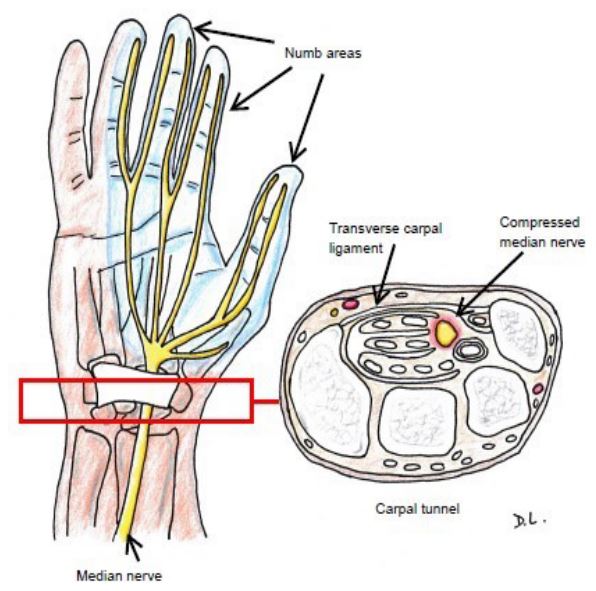
Carpal tunnel syndrome (compression of the median nerve
at the wrist)
CTS was first described by Sir James Paget in 1854 [2], in a
man who developed pain and impaired sensation in the hand,
from the trauma of a cord drawn tightly around his wrist. It is
by far, the most frequent EN, not only of the MN, but of all the
rest of EN taken together. It affects about 2 to 3% of the total population [3], and accounts for more than one half of all
the EN. Its pathogenesis is the compression of the MN by the
transverse carpal ligament at the wrist. The main symptoms are paresthesias and/or pain in the territory of distribution of the
MN (in palmar side, thumb, index, middle fingers and the radial side of the ring finger). These symptoms worsen at night
and upon awakening (at night, wrist had been in hyperflexion
or hyperextension) [4]. Patients try to shake their hands or rub
them (Flick´s syndrome) [5]. Nevertheless, the palm sensation
is not completely lost, as the palm is innervated by the palmar
cutaneous branch, which does not pass through the carpal tunnel. Therefore, if the palmar sensation is lost, the nerve injury
is more proximal to the carpal tunnel. On physical examination,
percussion on the MN in the carpal tunnel, elicit a sensation of
tingling in the distribution of the MN (Tinel´s sign), as we can
see in Figure 1. A provocation test that may help in the diagnosis
of CTS, consists in increasing the pressure in the carpal tunnel,
for example, if the patient hyperflexes the wrist. In the Phalen´s
test, the patient holds his wrists in complete and forced flexion (with the dorsal surfaces of both hands together) for up to
one minute. If the patient starts feeling the typical CTS symptomatology (paresthesias over MN distribution in the affected
hand), then the test is positive (abnormal). Another provocative
test over the carpal tunnel is the carpal compression test (Durkan’s test). The clinician compresses the MN with his own fingers until his nail bed whitens, for 30 seconds, on the patient´s
proximal wrist crease. If the patient feels pain or paresthesia
in the MN distribution, then the result is positive. When CTS is
long term, patients may have weakness in the hand and thenar
eminence atrophy. The diagnosis of CTS can be done with Nerve
Conduction Studies (NCS) that may show mainly the functionality of the nerve, if demyelination is present. Image techniques
can be also be used, above all Ultrasonography (US), or in rare
cases Magnetic Resonance Imaging (MRI). Regarding CTS treatment, the most useful treatments are splints, local injections of
corticosteroids and decompressive surgery [6,7]. Splints can be
prescribed for every patient, local injections for patients with
less severe symptoms, and decompressive surgery when the
symptoms are longer or more severe, and definitely when there
is a thenar eminence atrophy or severely impaired NCS [8,11].
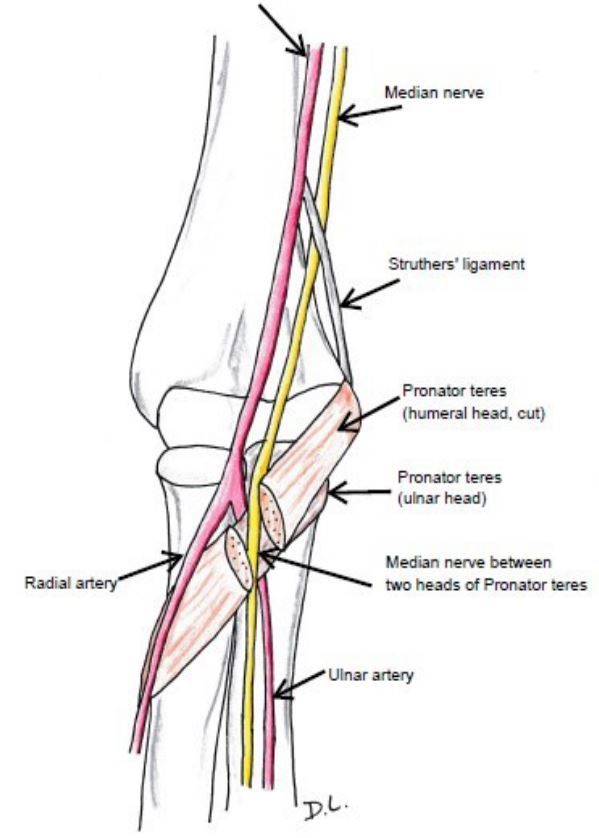
Pronator teres syndrome (also called pronator syndrome)
The Pronator Teres Syndrome (PTS) was first described by
Henrik Seyffarth in 1951 [12]. Behind the CTS, PTS is by far the
next more frequent MN entrapment syndrome. PTS is a rare
condition, it accounts for <1 per 100,000 annually. Its pathogenesis consists of the MN compression between the humeral
and ulnar head of the pronator teres muscle. Usually there is a
fibrous band between both heads (Figure 2).
The main symptoms of PTS include paresthesias in the distribution of the MN, similar to CTS, but not preferent nocturnal
or when in bed. The pain is more on the proximal volar forearm
region, about 5 cm proximal to the carpal tunnel [12]. On physical examination, we can basically practice three maneuvers to
evaluate the PTS [13]. The first one is the pronator compression
test, probably the most reliable. We apply 30 seconds of pressure proximally and laterally to the proximal edge of the pronator teres muscle belly. If the pain or paresthesia is reproduced,
then the test is positive. The second test is the resisted pronation/supination. With the patient´s affected elbow in 90 degrees of flexion, we stabilize with one hand the patient´s elbow,
while the other hand grasps the patient´s hand as in handshake
position. The patient keeps his forearm in a neutral position,
whilst the examiner supinates the patient’s forearm, explaining
to the patient to actively resist this movement. This will force
their pronator muscles (as they try to move into pronation).
While holding the resistance against pronation, the examiner
extends the patient’s elbow. The test is positive if the pain is reproduced. The patient´s elbow should be relaxed, otherwise, if
it is kept firmly in flexion, the elbow extension will not be possible. The last test is the resisted flexion of the proximal interphalangeal joint of the middle finger. This test will reproduce pain
and paresthesia when the MN is trapped at the heads of the
flexor digitorum superficialis muscle. As in CTS, Tinel sign can be
also positive, but it should be in the proximal anterior forearm
area, not above the carpal tunnel, as in CTS. Phalen´s test can
be positive up to one half of PTS. Nevertheless, muscle atrophy
is very uncommon in PTS. All these signs and symptoms may
be very confusing because a CTS or an epitrochleitis (golfer´s
elbow) can coexist with PTS. The diagnosis of PTS is very challenging, a great dose of clinical suspicious, based upon the clinical history, is needed. Plain x-rays are mandatory, and it should
be the first step to diagnosis, to rule out other processes. NCS
are also recommended, despite they are not usually diagnostic.
They are very useful in excluding coexisting pathology, usually
CTS. Image techniques as US and MRI can also be very helpful.
They can show direct causes as invasive lesions, cysts, tumors
or anatomical variants. The PTS treatment is usually conservative in most of the cases. Local rest, anti-inflammatories and
oral corticosteroids can be useful. Splints can be useful as well,
to avoid forearm rotation. In refractory cases or in space-occupying lesions, surgical decompression of the area is indicated
and it is highly effective. Very likely, due to similar clinical presentation, many authors include in the term PTS, three other
anatomical regions where the MN can be compressed in the
forearm (besides the pronator teres muscle, sensu stricto): 1)
Lacertus fibrosus, 2) Ligament of Struthers, and 3) Fibrous arch
of flexor digitorum superficialis [12]. In Table 1: we have them
schematically.
Table 1: Most frequent anatomical places of median nerve entrapment in the elbow.
| Syndrome |
Structure |
Location |
Extending from |
| Pronator teres |
Muscle |
Bellow elbow |
The two heads of the
Pronator teres muscle
|
| Lacertus fibrosus |
Fibrous |
Roof over forearm muscles
|
Biceps tendon |
| Ligament of Struthers |
Ligament |
Above elbow |
Humerus |
| Sublimis bridge |
Tendinous or muscle |
Upper forearm |
Inserting in upper forearm,
finger flexion
|
|
Anterior interosseous nerve
|
Tendinous or muscle |
Upper forearm |
The two heads of the
Pronator teres, downwards
|
| Carpal tunnel |
Fibrous/Ligament |
Wrist |
Pisiform & hamate bones
to scaphoid & trapezium
|
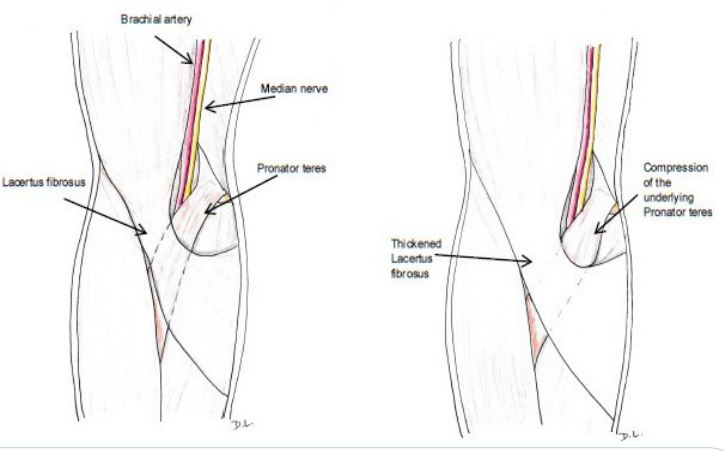
A compression of the MN at any of the above sites, many
authors just refer to them collectively as Pronator Teres Syndrome. 1) MN entrapment by hypertrophied bicipital aponeurosis or lacertus fibrosus, it is known as Lacertus syndrome.
Lacertus fibrosus is a ligamentous tissue attaching the biceps
to the ulna, over the MN in the proximal forearm (Figure 3).
Despite the compression location is not exactly the same in LS
than in PTS, the symptoms, physical examination, diagnosis and
treatments are very similar [15,16]. The pain in the forearm and
paresthesias in the median-innervated digits is exacerbated by
resisted flexion of the elbow with the forearm in supination.
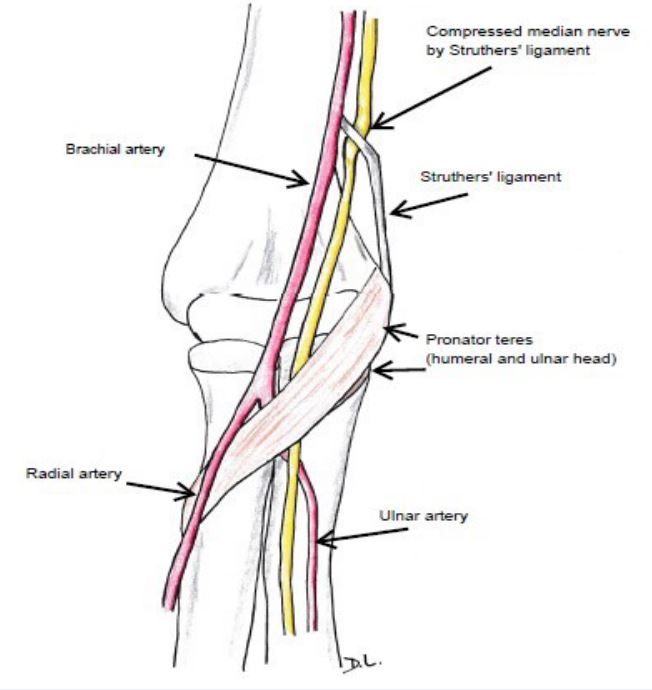
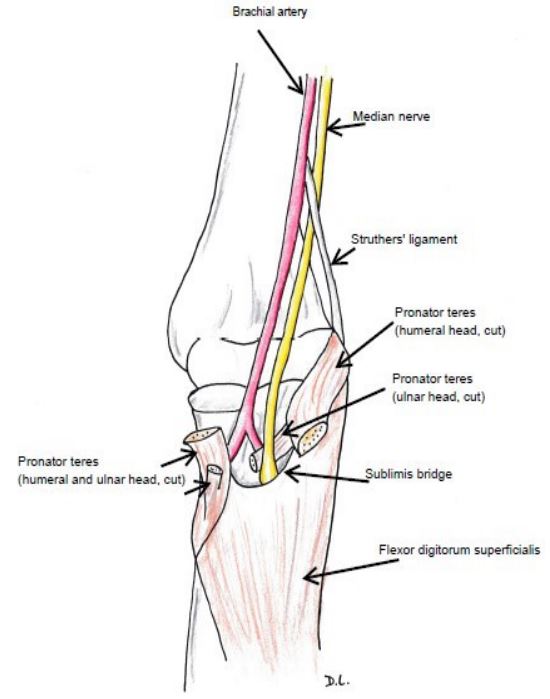
2) MN can also be compressed by the ligament of Struthers,
and this is called supracondylar process syndrome, or Struthers
syndrome, being extremely rare. This ligament is a fibrous band
running from the supracondylar process of the humerus to
the junction of the medial humeral epicondyle (Figure 4). The
pain in the forearm and paresthesias in the median-innervated
digits [17]. The most frequent symptoms are pain in the fore- pain in the fore- pain in the forearm (worsened by extension of the wrist) and paresthesias in
the distribution territory of the MN in the hand. On physical exam, the pain in the forearm is exacerbated by supination of
the forearm and extension of the elbow (versus pronation in
PTS) [17]. Because the brachial artery runs next to the median
nerve, occasionally the radial pulse may also be decreased. This
syndrome is very difficult to diagnose, and usually, only surgical
exploration of the nerve can identify the structure responsible
for nerve compression.
3) MN compressed at the fibrous arch of the origin of the
flexor digitorum superficialis passing between its humeral and
ulnar heads (sublimis bridge or arcade of Fearn and Goodfellow) (Figure 5). The pain in a forearm and paresthesias in the
median-innervated digits is exacerbated by resisted flexion of
the proximal interphalangeal joint of the middle finger while
other fingers are held in extension.
Table 2: Main characteristics of the most frequent entrapment neuropathies of the median nerve.
|
Carpal tunnel syndrome |
Pronator teres syndrome |
Anterior interosseous nerve
syndrome
|
| First description Year |
James Paget 1854 |
Henrik Seyffarth 1951 |
Parsonage and Turner 1948
|
| Frequency |
The most frequent of all.
2.5%
|
Rare <1/100.000 |
Very rare |
| Predisposing factors |
Repetitive movements
Hypothyroidism
Diabetes
mellitus
|
Repetitive movements
Hypothyroidism
Diabetes
mellitus
|
Traumatic.
Compression
and brachial plexus
neuritis.
|
| Location |
Wrist |
Elbow |
Elbow |
| Compression by: |
Transverse carpal ligament
|
Humeral and ulnar head of
the pronator
teres
muscle
|
Usually, it is the tendinous
edge of the deep
head
of the pronator teres
muscle.
|
| Symptoms |
Paresthesias, pain in wrist
and palm
|
Tenderness over the pronator
teres muscle.
Pain with
resisted pronation of the
forearm.
Weakness with
abduction of the thumb
|
Only motor deficiency:
isolated paralysis of
the
AIN-supplied muscles:
weakness of the
index
and thumb finger pincer
movement.
|
Compression eliciting
(or
worsening) numbness
|
Above the carpal tunnel
(Durkan´s test)
|
Over the pronator region
|
Negative |
| Physical examination |
Tinel, Phalen, Durkan Thenar
eminence
atrophy
|
Pronator compression test.
Resisted prona-
tion/supination.
Resisted flexion of the
proximal
interphalangeal joint of the
middle
finger.
|
Pinch grip test + Unable to
do “OK” sign
Difficult
fist inability to button
their shirts
|
| Diagnosis |
Nerve conduction studies
Echography,
MRI
|
Nerve conduction studies.
Echography,
MRI
|
Nerve conduction studies.
MRI
|
| Treatment |
Wrist splint
Local
corticosteroid injection
Surgery
|
Splints
Physiotherapy
Surgery
|
Splints
Physiotherapy
Surgery
|
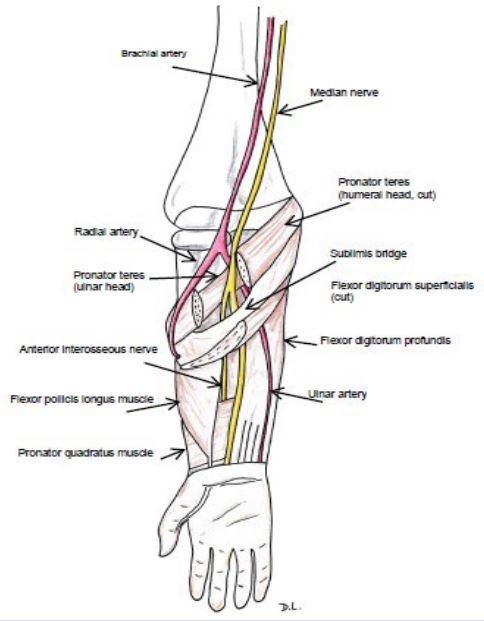
Anterior interosseous nerve syndrome (Kiloh-Nevin Syndrome):
The Anterior Interosseous Nerve Syndrome (AINS) is an extremely rare EN of the MN. It was first described by Parsonage
and Turner in 1948 (do not mistake with the Parsonage-Turner
syndrome, also known as brachial plexus neuritis or neuralgic
amyotrophy). The location of the EN of the AINS are usually the
tendinous origin of the flexor digitorum superficialis muscle,
at an accessory head of the flexor pollicis longus muscle, and at the tendinous origin of the deep head of the pronator teres
muscle (Figure 6) [18].
The AIN is the last major branch of the MN, leaving about 5
to 8 cm distal to the lateral epicondyle. AINS is an exclusively
motor EN of the MN, affecting three muscles in the forearm
(the flexor pollicis longus, flexor digitorum profundus and pronator quadratus).
The main symptoms are motor weakness, with difficulties
to pinch the thumb and index finger together. On a physical
examination these patients fail to make an “OK” sign with the
hand, because of the weakness (palsy) of the flexor pollicis longus muscle and flexor digitorum profundus muscle to the index
finger, with a positive Pinch Grip test (Froment’s sign). Instead
the “OK” sign, the patient will only be able to clap the sheet
between the index finger and an extended thumb [19].
When the patient is requested to make a fist, the flexion
of index and middle finger will be impaired, showing hand of
benediction. Do not mistake this sign with the claw hand from
ulnar neuropathy [19].
Clinically, there is no sensory loss in AINS, as it carries only
deep sensory fibers to the wrist.
NCS will show no changes in sensory parameters, as there
is no sensory innervation in this nerve. Nonetheless, they will
show findings in the flexor pollicis longus, the radial portion
of the flexor digitorum profundus, and the pronator quadratus. Nevertheless, in a thorough study, Pham et al [20] could
not demonstrate these findings. Furthermore, they saw that
at least their NCS showed non-localizing nerve damage. They
could not discriminate between injury to the AIN itself and a
more proximal lesion. They even suggested that because of the
predominance of lesions at upper arm level in their patients, it
could be supposed that AINS is not an entrapment neuropathy.
MRI can be also very helpful.
Regarding treatment of AINS, oral anti-inflammatories, short
term corticosteroids and physiotherapy should be indicated in
first term. If no better, then surgical treatment is of choice.
References
- https://emedicine.medscape.com/article/249784-clinical Hanna AS, Fried TD, Ghobrial GM et al. Nerve Entrapment Syndromes. 2023.
- Pfeffer GB, Gelberman RH, Boyes JH, Rydevik B. The history of carpal tunnel syndrome. J Hand Surg Br. 1988; 13(1): 28-34. DOI: 10.1016/0266-7681_88_90046-0. PMID: 3283274.
- Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosén I. Prevalence of carpal tunnel syndrome in a general population. JAMA. 1999; 282(2): 153-158.
- Joshi A, Patel K, Mohamed A, Solomon O, Zhang MH, Hsiung H et al. Carpal Tunnel Syndrome: Pathophysiology and Comprehensive Guidelines for Clinical Evaluation and Treatment. Cureus. 2022; 14(7): 27053. [QxMD MEDLINE Link].
- Hansen PA, Micklesen P, Robinson LR. Clinical utility of the flick maneuver in diagnosing carpal tunnel syndrome. Am J Phys Med Rehabil. 2004; 83(5): 363-367. DOI: 10.1097/01.phm.0000124439.14757.99. PMID: 15100625.
- Ly-Pen D, Andreu JL. Tratamiento del síndrome del túnel carpiano (Carpal tunnel syndrome treatment). Med Clin (Barc). 2005; 125: 585-589. DOI:10.1157/13080654.
- Goyal R, Kaneria J, Rai MK, Bhutani MK, Singh R, Rana P. Efficacy of Surgical Vs. Non-Surgical Treatment of Carpal Tunnel Syndrome (CTS): A Systematic Review. Value Health. 2015; 18: 635. DOI:https://doi.org/10.1016/j.jval.2015.09.2255.
- Ly-Pen D, Andréu JL, de Blas G, Sánchez-Olaso A, Millán I. Surgical decompression versus local steroid injection in carpal tunnel syndrome: a one-year, prospective, randomized, open, controlled clinical trial. Arthritis Rheum. 2005; 52(2): 612-619. DOI:10.1002/art.20767.
- Ly-Pen D, Andréu JL, Millán I, de Blas G, Sánchez-Olaso A. Comparison of surgical decompression and local steroid injection in the treatment of carpal tunnel syndrome: 2-year clinical results from a randomized trial. Rheumatology. 2012; 51(8): 1447-1454. DOI: 10.1093/rheumatology/kes053.
- Ly-Pen D, Andreu JL, Millán I, de Blas G, Sánchez-Olaso A. Long-term Outcome of Local Steroid Injections Versus Surgery in Carpal Tunnel Syndrome: Observational Extension of a Randomized Clinical Trial. Hand (N Y). 2022; 17(4): 639-645. DOI: 10.1177/1558944720944263. Epub 2020 Aug 6. PMID: 32757777; PMCID: PMC9274889.
- Shi Q, Bobos P, Lalone EA, Warren L, MacDermid JC. Comparison of the Short-Term and Long-Term Effects of Surgery and Nonsurgical Intervention in Treating Carpal Tunnel Syndrome: A Systematic Review and Meta-Analysis. HAND. 2020; 15(1): 13-22. DOI:10.1177/1558944718787892
- Dididze M, Tafti D, Sherman AI. Pronator Teres Syndrome. StatPearls, NCBI Bookshelf. 2023. https://www.ncbi.nlm.nih.gov/books/NBK526090/.
- Sullivan A. Pronator Teres Syndrome Test. Edited . Arkansas Colleges of Health Education School of Physical Therapy Musculoskeletal 1 Project. 2023. https://www.physio-pedia.com/Pronator_Teres_Syndrome_Test.
- Mehl A, Stevenson J, Royal JT, Lourie GM. Lacertus syndrome: Use of pre-and post-exercise MRI to aid in diagnosis and treatment. Radiology Case Reports. 2021; 16(5): 1113-1117.
- Ahmad AA, Abdullah S, Thavamany AS, Tong CY, Ganapathy SS. Lacertus Syndrome: an Outcome Analysis After Lacertus Release. JHS GO. 2023.
- Hagert E, Jedeskog U, Hagert CG, Fermín TM. Lacertus syndrome: a ten-year analysis of two hundred and seventy-five minimally invasive surgical decompressions of median nerve entrapment at the elbow. Int Orthop. 2023; 47(4): 1005-11. DOI: 10.1007/s00264-023-05709-w. Epub 2023 Feb 9. PMID: 36757413; PMCID: PMC10014674.
- Tang JB. Ligament of Struthers: exceedingly rarely causes ulnar neuropathy and exploration is not suggested in cubital tunnel syndrome. J. Hand Surg. Eur. 2021; 46(7): 800-805. DOI:10.1177/17531934211026408
- Rabaut V, Van de Vyver V, Verstraete K. Kiloh-Nevin Syndrome. J Belg Soc Radiol. 2020; 104(1): 49. DOI: 10.5334/jbsr.2183. PMID: 32964190; PMCID: PMC7485407.
- Meyer P, Lintingre PF, Pesquer L, Poussange N, Silvestre A, Dallaudière B. The Median Nerve at the Carpal Tunnel … and Elsewhere. J Belg Soc Radiol. 2018; 102(1): 17. DOI: 10.5334/jbsr.1354. PMID: 30039031; PMCID: PMC6032467.
- Pham M, Bäumer P, Meinck HM, Schiefer J, Weiler M, Bendszus M, et al. Anterior interosseous nerve syndrome. Fascicular motor lesions of median nerve trunk. Neurology 2014; 82(7): 598-606; DOI: 10.1212/WNL.0000000000000128.