Introduction
Mature cystic teratomas (MCTs) primarily demonstrating
skin structures of ectodermal origin may be referred to as dermoid cysts. Dermoid MCTs have a characteristic keratinized
squamous epithelial lining, frequently punctated by hair follicles, with hairs directed into the cystic lumen or the lining itself
[1,2]. Intramural adnexal structures, including eccrine and sebaceous glands, may drain their contents into the lumen, accumulating sebum, keratin, and hair [3]. Giant cell reactions and focal
calcifications may also be present [2,4]. At smaller sizes, MCTs
may be asymptomatic, incidental findings [5,6]. Mass effects account for most symptoms as the teratomas gradually grow, with
the exact manifestation dependent on their location and extent
[7]. Patients with MCTs in the abdomen may report progressive abdominal pain and distention, urinary issues, neurological symptoms, or infections [6-8]. Rupture may lead to further
complications, such as chemical peritonitis [6]. Dermoid cysts
and other MCTs are typically benign, though the development
of malignancies, including squamous cell carcinoma, has been
reported [6,9]. Resection is the standard treatment and is also
necessary for the histopathological confirmation of the diagnosis [6,10]. We herein present, to our knowledge, the third documented manifestation in English literature of an extragonadal
intramuscular dermoid MCT within the pelvic musculature in a
male patient, not associated with the presacral space. Extragonadal MCTs in the adult male are a rarity; those within the male
pelvis are even more so. A literature search for intramuscular
dermoid cysts in the pelvis returned three cases, all in male patients [2,8,11,14]. In contrast to previous instances, which had
extensions of the tumor through the levator ani, the present
case appeared centered in the obturator internus. This report
may prove valuable in expanding the differential diagnosis for
similar lesions in the pelvic region. Moreover, the recurrence of
the cyst supports the importance of high vigilance during surgical removal to achieve a complete resection of such tumors.
Case presentation
A 30-year-old male presented to the ER with pain in his left
hip and abdomen. A CT scan revealed a large pelvic mass of unclear etiology. He was referred to orthopedic oncology, where
his initial diagnosis was suspected to be an unusual synovial
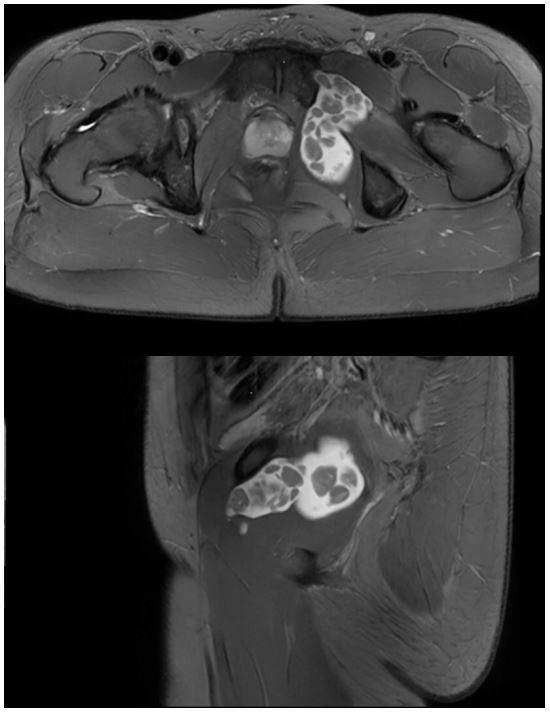
chondromatosis. Multisequence multiplanar MRI revealed an
indeterminate, intramuscular cystic mass measuring, along its
greatest dimension, 7.0 cm in the transverse plane. Spanning
through the obturator foramen, the mass involved the body of the left obturator internus, the obturator externus, and the
adductor compartment. Viewed with T1 weighting, faint peripheral enhancement of the cyst was observed. It appeared to
contain multiple solid bodies, which were mildly hyperintense
with T1 weighting and suppressed on fat-saturated sequences.
Prohance contrast images did not enhance the bodies (Figure
1). Open resection of the mass was pursued through a retropubic approach via a Pfannenstiel incision to reach the involved
pelvic musculature. Adherence to the iliac vesicles, bladder
wall, prostate, rectum, internal iliac, obturator vessels, and local
nerves made for a challenging surgery, and intraoperative rupture occurred. Cystic contents included abundant hair in a yellow, noncellular fluid. Frozen sections obtained during surgery
suggested a potential mature teratoma, and the remainder of
the specimen was submitted entirely for permanent diagnosis.
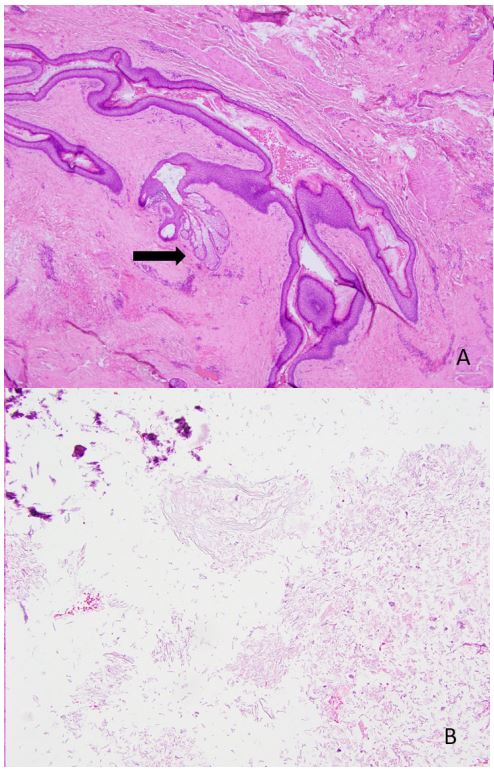
Viewed under microscopic examination with hematoxylin and
eosin staining, the cyst wall contained keratinized squamous
epithelium with several sebaceous glands and hair follicles (Figure 2). As mesodermal- and endodermal-derived structures
were absent, the diagnosis of a dermoid MCT was favored. The
patient reported pain relief immediately after surgery. However, within two months, he experienced a recurrence of abdominal pain, pain radiating down his left leg, as well as loss of
appetite, nausea, bloating, changes in stooling frequency, and
difficulty urinating. MRI showed an increasing fluid component
of a recurred cyst extending from the obturator fossa into the
pelvis. Potential residual teratomatous lesions were postulated.
A fluid collection in the surgical cavity with a hypoechoic nodule at the left epididymal tail, hyperemia of the left epididymis,
and small bilateral hydroceles were also noted. Given the rapidity of its growth and the return of the patient’s pain, resection
was once again sought. The robot-assisted laparoscopic excision
achieved a visually complete removal of the cyst and cyst wall in
three distinct segments. Histopathological examination of the
mass demonstrated the same features as the initial excision, including a cyst with a lining of stratified squamous epithelium,
in addition to fibrous and granulation tissue. Within six weeks,
abdominal pain complicated the patient’s course. Follow-up CT
findings of a gas and fluid collection in the surgical bed were
concerning for an abscess, which was subsequently drained.
Discussion
Teratomas are germ cell tumors that can contain derivatives
of all three embryonic germ layers. The etiology is uncertain,
and the exact mechanism may vary by location [15]. Many theorize that they stem from aberrant primordial germ cells that
have strayed from their normal migratory path [16]. They may
be classified as either mature, if they contain less than 10%
undifferentiated tissue, or immature [6]. Additionally, the contents may be used to classify teratomas as either solid, cystic, or
mixed. Immature and solid teratomas tend to present relatively
greater potential for malignancy [6]. Mature cystic teratomas
(MCTs) contain differentiated tissues derived from at least two
of the three embryological germ layers. Dermoid cysts are MCTs
that contain primarily ectoderm-derived skin structures. While
ovarian dermoid cysts are the most common MCT in adults,
extragonadal manifestations also exist [17]. MCTs in the retroperitoneal space are rare, accounting for less than 3% to 5%
of all teratomas [18,20]. This space is confined by the posterior parietal peritoneum and the posterior body wall, with the diaphragm forming the superior boundary and the pelvic diaphragm at the inferior extent [21]. Here, MCTs are diagnosed
most often within the first year of life, though a second peak
of incidence occurs in young adulthood, with only 10% to 20%
of cases reported in patients older than 30 [6,22]. They occur
in females roughly two to three times as often as in males [19,
22]. Thus, few reports of dermoid cysts in the adult male pelvis exist [19,22]. The present case is notable for three main aspects: (i) its rarity as an intramuscular dermoid MCT in the male
pelvis, (ii) its potential to expand the differential diagnosis for
masses of the pelvic musculature, and (iii) its rapid recurrence
in the context of incomplete resection and intraoperative rupture. The site and muscular involvement of the current case are
unique. It has no presence in the presacral space but rather is
situated anterolateral to the rectum. This distinguishes it from
type IV sacrococcygeal teratomas, which occupy the presacral
space posterior to the rectum and anterior to the sacrum [7].
A PubMed search of English literature for extragonadal dermoid MCTs in the pelvis anterior to the rectum returned four
cases [2,11,13,14]. The intramuscular nature of the mass further distinguishes it. Three of the four previous reports of intramuscular dermoid cysts outside of the orbit involve pelvic
muscles. Tanaka et al. describe a case in the erector spinae in a
67-year-old male [5]. Lukanovic and Patrelli describe a 24-yearold female with a paravesical mass that contacted the obturator internus, extended to the ischiorectal fossa, and integrated
with the levator ani [11]. Choudur et al. and Van Gelderen et al.
likewise describe pelvic dermoid cysts with extensions through
the levator ani in two male patients [12,13]. None of these instances replicate the anatomy of the present case, which centered within the obturator internus and involved the obturator foramen, obturator externus, and adductor compartment,
with adhesions to the bladder, prostate, and rectum. While
little precedent exists for a dermoid MCT occurring with this
anatomical involvement, radiological and pathological evidence
support the diagnosis. Magnetic resonance imaging of a dermoid MCT often reveals a hyperintense mass on T2-weighted
imaging [5,23,24]. The mass characteristically contains several
smaller bodies less intense than the surrounding cystic fluid.
Some refer to this appearance as a “sack of marbles” [5,25].
T1-weighted imaging may show somewhat hyperintense nodules compared to the surrounding fluid [5,23,24]. Fat saturation
suppresses the intensity of the nodules in T1-weighted images,
supporting a fatty composition [5]. This description aligns well
with the MRI results for this case. The pathological report likewise indicates a dermoid MCT. No undifferentiated cells were
observed, and ectodermal skin structures primarily were seen,
as noted in a previously documented dermoid MCT in the male
pelvis [2]. The differential diagnosis for a cystic mass in this region includes hydatid cyst [26], epidermoid cyst [27], mycetoma
[4], liposarcoma [28], hematoma, sarcoma, and carcinoma.
Notably, the literature is inconsistent in the discrimination, or
lack thereof, between the often subcutaneous dermoid cysts
and dermoid MCTs. Some authors make a distinction based on
origin and the potential to find structures from multiple germ
layers. In this classification, dermoid MCTs, which develop from
primordial germ cells, are lesions of mostly ectoderm-derived
structures, with minimal presence of other germ layers [29].
Dermoid cysts, as commonly occur on the face of neonates,
arise specifically from entrapped ectoderm, with more limited
potential for differentiation [30,31]. Alternatively, some view all
dermoid cysts as a subcategory of mature cystic teratomas [11].
Due to the extreme rarity of intramuscular MCTs, the effect of muscular involvement on the recurrence risk is not well
defined. Incomplete resection increases the recurrence rate
among sacrococcygeal teratomas and ovarian dermoid cysts
[7,10,32]. Recurrence may be especially high in sacrococcygeal
teratomas due to the relatively high frequency of incomplete
capsules and the potential for the coccyx to harbor residual totipotent cells [7]. Similarly, the interaction of muscle with the
dermoid cyst may have played a role in the recurrence observed
in this case. Rupture may also be associated with an increased
risk for benign recurrence, as noted in ovarian dermoid cysts
[33]. As the initial resection was incomplete and intraoperative
rupture occurred, the rapid recurrence cannot be attributed
with certainty to the intramuscular character of the teratoma
[33]. The potential interaction between intramuscular location
and recurrence risk requires further investigation.
Conclusion
Dermoid MCTs in the male pelvic retroperitoneum are extremely rare, and those in the pelvic musculature are even
more so. This report documents what is, to our knowledge,
the first occurrence of an intramuscular dermoid MCT within
the obturator internus. We aim for this rare case to heighten
awareness about this tumor’s rarity, broaden the spectrum of
differential diagnoses concerning retroperitoneal intramuscular
tumors, and underscore the significance of complete resection
during surgery.
References
- McKenney JK, A Heerema-McKenney, RV Rouse. Extragonadal germ cell tumors: a review with emphasis on pathologic features, clinical prognostic variables, and differential diagnostic considerations. Adv Anat Pathol. 2007; 14(2): 69-92.
- Chalhoub K, et al. Primary Mature Cystic Teratoma Compressing the Prostate in a 28-Year-Old Male: A Case Report and Literature Review. Case Rep Urol. 2019; 2019: 8970172.
- Cong L, et al. Mature Cystic Teratoma: An Integrated Review. Int J Mol Sci. 2023; 24(7).
- Tiu A, et al. Primary retroperitoneal mature cystic teratoma (dermoid cyst) in a 51-year-old male:Case report and historical literature review. SAGE Open Med Case Rep. 2017; 5: 2050313-17700745.
- Tanaka T, et al. Dermoid cyst presenting as an intramuscular mass: CT and MRI features. Diagn Interv Imaging. 2019; 100(3): 195-196.
- Gatcombe HG, et al. Primary retroperitoneal teratomas: a review of the literature. J Surg Oncol. 2004; 86(2): 107-13.
- Guo JX, JG Zhao and YN. Bao, Adult sacrococcygeal teratoma: A review. Medicine (Baltimore). 2022; 101(52): 32410.
- Alhumayed M and J. Liau, Extensive mature cystic teratoma in the pelvis of an adult male patient mimicking a prostatic abscess. Radiol Case Rep. 2021; 16(6): 1343-1347.
- O’Donovan EJ, K Thway and EC. Moskovic, Extragonadal teratomas of the adult abdomen and pelvis: a pictorial review. Br J Radiol. 2014; 87(1041): 20140116.
- Simpson PJ, et al. Surgical outcomes in adults with benign and malignant sacrococcygeal teratoma: a single-institution experience of 26 cases. Dis Colon Rectum. 2014; 57(7): 851-7.
- Lukanovic A and TS. Patrelli, Retroperitoneal mass with ischiorectal fossa extension: diagnosis, clinical features and surgical approach. A literature review starting from a rare clinical case of primary retroperitoneal dermoid cyst. Eur J Gynaecol Oncol. 2010; 31(6): 709-13.
- Choudur HN, et al. Unusual presentation of a dermoid cyst in the ischiorectal fossa. Magnetic resonance imaging and ultrasound appearances. Skeletal Radiol. 2009; 38(9): 921-4.
- Van Gelderen WF, et al, Radiological imaging of a massive dermoid in the male pelvis. Australas Radiol. 1995; 39(4): 408-10.
- Wilson RG, Dermoid cyst of the rectovesical space: report of a case. Dis Colon Rectum. 1973; 16(6): 530-1.
- Mosbech, C.H., et al., Recent advances in understanding the etiology and pathogenesis of pediatric germ cell tumors. J Pediatr Hematol Oncol. 2014; 36(4): 263-70.
- Mamsen LS, et al. The migration and loss of human primordial germ stem cells from the hind gut epithelium towards the gonadal ridge. Int J Dev Biol. 2012; 56(10-12): 771-8.
- Saida T, et al, Ovarian and non-ovarian teratomas: a wide spectrum of features. Jpn J Radiol. 2021; 39(2): 143-158.
- Tapper D and EE Lack, Teratomas in infancy and childhood. A 54-year experience at the Children’s Hospital Medical Center. Ann Surg. 1983; 198(3): 398-410.
- Grosfeld JL and DF. Billmire, Teratomas in infancy and childhood. Curr Probl Cancer. 1985; 9(9): 1-53.
- Isaacs H, Jr Perinatal (fetal and neonatal) germ cell tumors. J Pediatr Surg. 2004; 39(7): 1003-13.
- Chute R, SE. Leard and R Osgood, Primary retroperitoneal teratoma. J Urol. 1953; 70(3): 520-5.
- Davidson AJ, DS. Hartman, and S.M. Goldman, Mature teratoma of the retroperitoneum: radiologic, pathologic, and clinical correlation. Radiology. 1989. 172(2): 421-5.
- Erden, A, et al. Retrorectal dermoid cyst in a male adult: case report. Abdom Imaging. 2003; 28(5): 725-7.
- Outwater EK, ES. Siegelman and JL Hunt, Ovarian teratomas: tumor types and imaging characteristics. Radiographics. 2001; 21(2): 475-90.
- Wong KT, et al. Imaging of cystic or cyst-like neck masses. Clin Radiol. 2008; 63(6): 613-22.
- Özdemir M, et al. Primary hydatid cyst in the adductor magnus muscle. BJR Case Rep. 2020; 6(3): 20200019.
- Sakurai T, et al. Laparoscopic resection for a relapsed presacral epidermoid cyst penetrating the ischiorectal fossa. Asian J Endosc Surg. 2022; 15(3): 656-659.
- Shanbhogue AK, et al. Uncommon primary pelvic retroperitoneal masses in adults: a pattern-based imaging approach. Radiographics. 2012; 32(3): 795-817.
- Brownstein MH and EB. Helwig, Subcutaneous Dermoid Cysts. Archives of Dermatology. 1973; 107(2): 237-239.
- Pear BL. Epidermoid and Dermoid Sequestration Cysts. American Journal of Roentgenology. 1970; 110(1): 148-155.
- Orozco-Covarrubias L, et al. Dermoid cysts: a report of 75 pediatric patients. Pediatr Dermatol. 2013; 30(6): 706-11.
- Multani J, S. Kives. Dermoid cysts in adolescents. Curr Opin Obstet Gynecol. 2015; 27(5): 315-9.
- Eisenberg N, et al. Short- and Long-Term Complications of Intraoperative Benign Ovarian Cyst Spillage: A Systematic Review and Meta-analysis. J Minim Invasive Gynecol. 2021; 28(5): 957-970.