Introduction
Ameloblastoma is well recognized as a locally invasive benign neoplasm thought to arise from the cellular components of
the enamel organ. Broca described ameloblastoma in 1868 [1].
Ameloblastoma contributes to about 1 % of all head and neck
tumors and 13 to 58% of all odontogenic tumors [2]. Maxillary
ameloblastoma is rare and account for 15% of all ameloblastomas. Slow-growing, painless swelling of the mandible or maxilla
is the most common presentation of ameloblastoma and the
diagnosis requires imaging (CT scan). Mutations in genes that
belong to the mitogen-activated protien kinase MAPK pathway
are found in many ameloblastomas, the most common being
the BRAFV600E mutation [3].
Case report
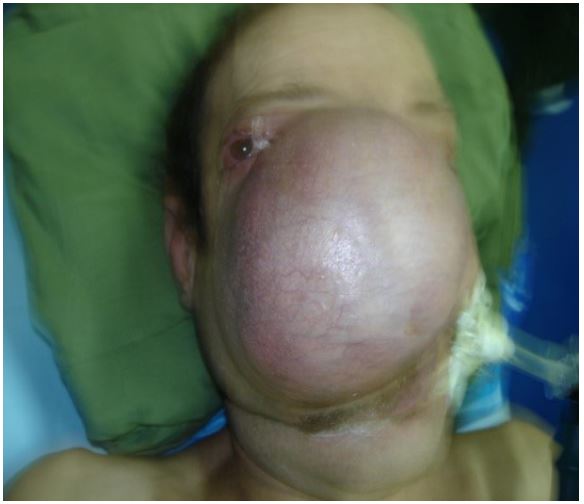
A 68-year-old man consulted in our ENT department with a
giant painless mass in the right hemi face since 15 years. This
lesion caused major cosmetic and psychological disturbance:
isolation and social difficulties. Inspection of face noted major
deformity by an ovoid swelling well- limited, non tender (Figure
1) extending to the lower orbital margin and involving the complete right side of the face. The skin was normal without ulceration or inflammation. Intra oral examination was normal. Nasal
endoscopy showed a normal mucous and internal displacement
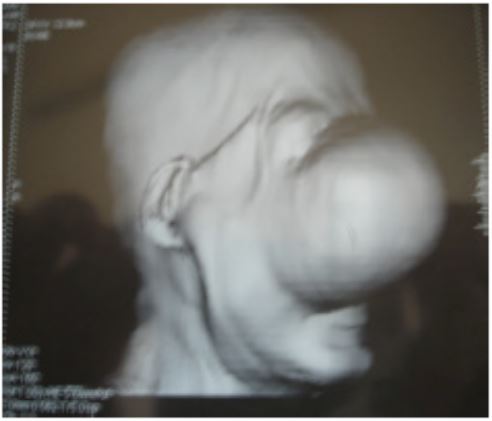
of the lateral side of the right nasal cavity. CT scan showed a
large heterogenic mass located on the right side of the face, invading the left left maxillary and ethmoidalsinus (Figure 2A,2B).
The patient classed stage II (Yang classification). After a discussion with the patient and his family we chose a surgical procedure by external or open approach. A lateral rhinotomy has occurred with a transfixed upper low and right vestibular incision.
A large hemi right facial flap was obtained, authorizing a well
exposing of the lesion. The mass was removed with a lateral
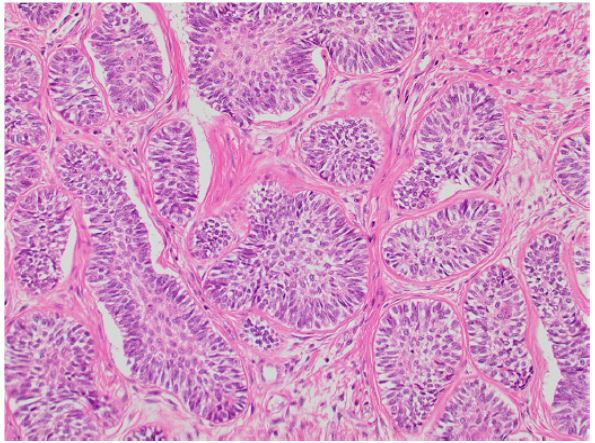
nasal wall The histopathologic study of the surgical specimens
confirmed the diagnosis of amelobalstoma without malignancy (Figure 3). Follow- up was full after 8 months, and the patient
has recovered social and relational activities (Figure 4).
Discussion
Sinonasal ameloblastomas are rare tumors of the sinonasal tract and show a predilection for the male gender with 59
years mean of age. Maxillary ameloblastoma is more aggressive
with a 50% rate of recurrence within 5 years of initial resection
[3]. It is generally a painless, slow growing, locally aggressive
tumor causing expansion of the cortical bone. The symptoms
include deformity (face or palatal deformity), headache, nasal
obstruction, epistaxis, intra oral ulceration (palatal ulceration).
The maxillary lesions and extensive lesions require CT and MRI
to establish the extent of the lesion. The biopsy confirms the
diagnosis and authorize reflection, and adaptable management
of the ameloblastoma case with case.
Yang suggested a classification based on diameter of tumor
and proposed three stages: stage I, the maximum tumor diameter ≤6 cm; stage II, the maximum diameter of tumor >6 cm
or tumor invasion into the maxillary sinus or orbital floor; and
stage III, tumor invasion of the skull base or metastasis into regional lymph nodes [4].
According to the new 2022 World Health Organization
(WHO) classification of ameloblastomas, they are classified in:
unicystic, extraosseous/peripheral, conventional, adenoid and
metastasizing ameloblastoma [5].
The histological varieties of ameloblastoma is important to
identifying because it was frequently associated with one or
multiples recurrences: granular cell ameloblastoma, follicular
and plexiform type [6].
The differential diagnosis include inverted papilloma (follicular and acanthomatous ameloblastoma), odontogenic fibromas,
non-keratinizing squamous cell carcinoma, adenoid cystic carcinoma, myeloma, sarcoma. The immunohistochemistry may be
help full and, all ameloblastoma cell express CK19 (odontogenic
epithelium marker) [6].
Recent advances report the detection of mutation in ameloblastomas interesting from newer treatment options. A
high incidence of BRAF V600E and SMO L 412F. The oncogenic
BRAFV600E mutation leads to the activation of mitogen-activated protein kinase (MAPK) pathway, which has resulted in successful treatment with BRAF inhibitor [7].
The challenge in managing ameloblastoma is in achieving
complete excision and reconstruction of the defect when the
tumor is large (Table 1).
Surgical resection is treatment of choice. Radical resection
with a margin of a least 1 to 2 cm is ideal to obtain save results.
Furthermore the radical treatment strategy is associated with a
higher risk of post operative complications and required numerous surgical operation (recurrence) and prosthetic procedures.
The quality of life of patients is significantly altered with pain
and local deformity. A conservative treatment, curettage, has a
recurrence rate of 60 to 80% [3,5].
Endoscopic sinus surgery can to be used in some selected
cases (karp). In 2021 Karp report only 2 cases in the literature
of endoscopic resection of ameloblastoma with respectively
4-year and 11 months follow-up [8,9].
Non-surgical treatment in ameloblastoma comported systemic chemotherapy (metastatic ameloblastoma) especially
platinum-based anticancer molecular. Recently molecular
targeted therapy was cited in many works: vemurafenib, dabrafenib and trametinib showed a notable reduction in tumor
volume [10].
Radiotherapy is utilized in select cases like residual disease
after surgery, multiple recurrences, impossibility of surgery or
unresectable lesions (66 to 70 Grays) [11].
The prognosis for ameloblastoma depends on the age of the
patient, location and size of the tumor, histological type, extent,
and stage of disease. The recurrence rate of 9,8% to 19,3% after
treatment, and more than 50% of recurrences occur within five
years of the primary surgical intervention.
Table 1: Ameloblastoma protocol of management.
| Section |
Modalities |
| Diagnosis |
Imaging: CT Scan.
Biopsy
(accessible lesion).
|
| Evaluation and Staging |
CT scan
MRI
Staging
(Yang classification)
|
| Therapeutic Protocol |
Surgical option
Radical
surgical resection with
margin (1.5-2 cm).
Reconstruction:
Flaps or Prosthetic
reparation
|
Post Operative
Evaluation
and Staging
|
Histopathologic study
-Histological
type
-Quality of
resection: margin
Identification
of prognosis factory
-Age
-Histological
variety
-Extension:
base of skull, orbit,
cerebral
-Recurrence
-Maxillary
or soft tissues extension
|
| Follow-Up |
CT Scan
Every 6 months
during 2 years.
|
Ameloblastoma with
Poor
Prognosis
|
Research of Mutation
Braf
V600E
|
Recurrence
1 OR 2 |
Gold Option
Surgical
Protocol (Radical
Resection).
|
| Multiples Recurrences |
Gold option: surgical
protocol
Option 2:
radiotherapy
Option 3:
targeted therapy
|
Metastatic
Ameloblastoma
|
Evaluation: TEP
Chemotherapy
Targeted
therapy
|
Conclusion
Ameloblastoma, an odontogenic tumor variety is rare with
a locally invasive potential, slow-growing with painless swelling
and deformity. CT scan shows the lesion, location and extension. The best treatment of ameloblastoma is surgical especially
in bloc resection (radical option). The future may be based on
molecular developments, with the possibility of targeted therapy.
References
- Martin Y, Sathyakumar M, Premkumar J, Magesh KT. Granular cell ameloblastoma. J Oral Maxillofac Pathol. 2017; 21(1): 183. doi: 10.4103/jomfp.JOMFP_45_15.
- Fregnani ER, da Cruz Perez DE, de Almeida OP, Kowalski LP, Soares FA, de Abreu Alves F. Clinicopathological study and treatment outcomes of 121 cases of ameloblastomas. Int J Oral Maxillofac Surg [Internet]. 2010; 39(2): 145-9.
- Sweeney RT, Mc Clary AC, Myers BR, Biscocho J, NeahringL, Kwei KA. Identification of recurrent SMO and BRAF mutations in ameloblastomas. Nat Genet. 46: 722-725. DOI 10.1038/hg.2986.
- Yang R, Liu Z, Gokavarapu S, Peng C, Ji T, Cao W. Recurrence and cancerization of ameloblastoma: multivariate analysis of 87 recurrent craniofacial ameloblastoma to assess risk factors associated with early recurrence and secondary ameloblastic carcinoma. Chin J Cancer Res. 2017: 189-95. 10.21147/j.issn.1000-9604.2017.03.04.
- Soluk-Tekkesin M, John M, Wright JM. The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2022 (5th) Edition. Turk Patoloji Derg. 2022; 38(2): 168-184. doi: 10.5146/tjpath.2022.01573.
- Ghai S. Ameloblastoma: An updated narrative review of an enigmatic tumor. Cureus. 2022; 14(8): 27734. doi: 10.7759/cureus.27734.eCollection2022 Aug.
- Kurppa KJ, Caton J, Morgan PR, et al. High frequency of BRAF V600E mutations in ameloblastoma J Pathol 2014; 232: 492 -8.
- Karp J, Xiong W, Derikvand S, Javer A. Maxillary Sinus Ameloblastoma: Transnasal Endoscopic Management. Ear Nose Throat J. 2021; 100(10): 908S-912S. doi: 10.1177/0145561320930555.
- Lee J, Ahmad ZA, Kim D, et al. Comparison between endoscopic prelacrimal medial mxillectomy and caldwell-Luc approach for benign maxillary sinus tumors. Clin Exp Otorhinolaryngol 2019; 12(3): 287-293.
- Kaye FJ, Ivey AM, Drane WE, Mendenhall WM, Allan RW. Clinical and radiographic response with combined BRAF-targeted therapy in stage 4 ameloblastoma. J Natl Cancer Inst. 2015; 107: 378. 10.1093/jnci/dju378.
- Koukourakis GV, Miliadou A, Sotiropoulou-Lontou A. Ameloblastoma, a rare benign odontogenic tumour: an interesting tumour review targeting the role of radiation therapy. Clin Transl Oncol. 2011; 13: 793-7. 10.1007/s12094-011-0735-5.