Introduction
A transverse vaginal septum is a Mullerian duct anomaly that
occurs when there is a congenital failure of the lower vaginal
central cells to generate. Severe cyclical abdominal pain can occur shortly after menarche. The retrograde menstrual flow can
cause peritoneal inflammation, adhesion, and even infertility.
This case series aims to describe the use of a modified corrugated stent and malecot catheter which has shown favourable
results in maintaining vaginal patency. The post-operative care
is always a challenge. Re-stenosis was extremely common and
poorly reported despite the greatest surgical procedures in
transverse vaginal septum, especially in high septum or thick
septum. The malekot catheter insertion not only serves as a
guide for future septum excision, but it can also self-prepare
the young child to conduct the dilation with continued counseling while the menses are still present. Despite the usual return
of menstruation based on the malekot catheter, the emphasis
on regular dilation remains crucial. According to specific institutional experiences in China, the catheter can be implanted for
up to three years without showing signs of infection.
Case report I
An eleven-year-old girl presented to the district hospital with
severe cyclical abdominal pain. There was a 24 week abdominal
mass. On perineal examination, there was only a dimple where
the vaginal opening was expected to be seen.
MRI revealed a transverse vaginal septum at the proximal
vagina with atretic distal vagina resulting in hematometra, hematotrachelos and bilateral hematosalphinx. An emergency
laparoscopy, drainage of the hematometra and hematotrachelos was performed to relieve her pain. Intra operatively, a huge distended 24 week size uterus and dilated cervix with bilateral
hematosalphinx was seen. An incision was made over the fundus of the uterus to insert the suction cannula and the collection was drained. About 700cc of stale blood was evacuated.
Post operatively, intramuscular medroxyprogesterone acetate
150 mg was given to suppress her menses while awaiting definitive surgery, planned for a month later.
Despite the medical suppression, the hematometra rapidly
reaccumulated. Definitive surgery was done laparoscopically.
A suction-irrigation cannula was inserted into the uterine cavity via an incision made at the uterine fundus. The probe was
pushed towards the vagina to help localize the margins and
plane of the transverse septum, thus helping to avoid bladder
and rectum injury. The surgery was performed with a Y incision
at the centre of the vaginal septum trans vaginally using the
suction-irrigation cannula as a guide. The septum was opened
up until the tip of the suction probe was visible. The thickness
of the transverse vaginal septum was estimated about 10 mm.
The mucosa flaps from the upper part of the vagina were pulled
downwards and sutured to underline the vaginal canal with
ecosorb 2/0 suture using the Z-plasty method.
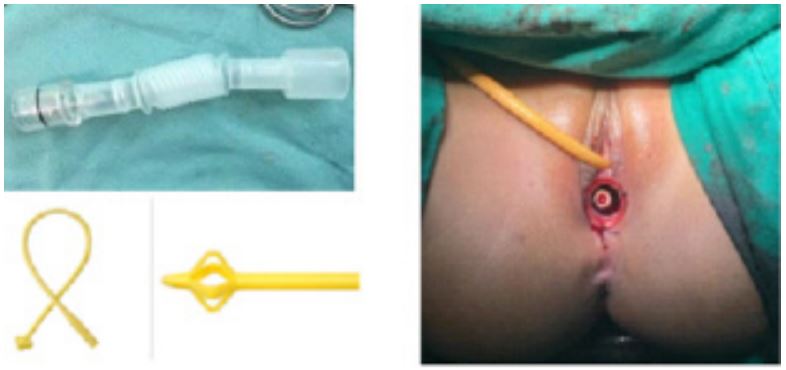
An endotracheal tube connector was modified to use only
the middle corrugated part (Figure 1) as a stent. The other parts
of the connector were cut at both ends and discarded. The
modified corrugated drain was covered with interceed (adhesion barrier) prior to its insertion in the vagina. It was secured
to the vulva with silk sutures which were removed a month
later. Subsequently, she was started on vaginal dilation under
supervision. The patient was fearful and experienced vaginal
discomfort and pain during dilation, resulting in re-stenosis due
to inadequate dilation.
About 4 months from the first vaginoplasty, she underwent
a second laparoscopy assisted vaginoplasty by the same team.
We performed the surgery in the same way as the first time but
decided to use a long term stent. We placed a malecot catheter whereby the 4 wings mushroom-shaped end was placed at
the fundus of uterus by pulling it through vaginal route using a
Maryland grasper that was inserted via an incision at the fundus
of the uterus; the other end of malekot catheter was excised at
the level of the introitus (Figure 1).
At 16 months post surgery, the patient was comfortable with
the malecot catheter in situ with return of monthly menses.
Case report II
An eleven-year-old student presented with intermittent colicky lower abdominal pain for one month. She was treated for a
urinary tract infection with antibiotics and analgesia but did not
improve. She had a tender 20 week size abdominal mass. Only
a vaginal dimple was seen upon examining the perineum. MRI
reported as transverse vaginal septum (0.9x1.3x0.2 cm) with
hematotrachelos and hematometra.
Laparoscopic drainage of hematometra and vaginal dilation
under anaesthesia was performed. Gradual vaginal dilation was
done over 5 months . She went through a repeat laparoscopic
drainage of haematometra when menstruation failed to be suppressed prior to definitive surgery.
Laparoscopy assisted vaginoplasty was subsequently performed in the same way as case one, however this time we inserted both the modified corrugated stent as well as the malecot catheter as there were concerns that she may not be able
to perform post operative vaginal dilation adequately. The stent was removed 2 weeks after the operation as she was in pain
while the malecot catheter was left in situ. She subsequently
had normal monthly menses. She started to dilate from about
2 weeks post surgery and the malecot catheter was removed
about 7 months after surgery.
Case report III
A fourteen-year-old girl complained of abdominal discomfort and left sided abdominal mass for one week. A 20 week
abdominal mass was noted. A hymenal ring was seen with no
obvious bulge beyond hymenal ring. MRI pelvis reported a hematometra and haematocolpos due to transverse vaginal septum which measured 12 mm in thickness.
She underwent a laparoscopic assisted vaginoplasty. The
thickness of the transverse vaginal septum was estimated to be
20 mm. Vaginal length was about 5 cm. The surgery was performed in the same way as the previous cases.
Case report IV & V
Similarly, a fourteen-year-old student and a ten-year-old
student presented with abdominal pain and were diagnosed to
have mid transverse vaginal septum. Surgery utilizing both corrugated stent and malecot catheter was performed. Post operatively, prophylactic antibiotic was given to all patients for two
weeks (Table 1).
Another case that utilized the modified corrugated stent
was excluded as she did not have outflow obstruction as highlighted in above young post menarchal patients. She was diagnosed to have incomplete mid transverse septum during her
fertility workup and she achieved spontaneous pregnancy three
months after the surgery done same way as described.
Table 1: Summary of transverse vaginal septum cases where a modified corrugated stent and malecot catheter was utilized.
| No |
Patients |
Intra-operative
Diagnosis
|
Imaging |
Intervention |
Outcome |
| 1 |
11 years old
|
High Transverse Vag-
inal
Septum -10 mm
with
Atretic Vaginal
|
MRI High transverse
vaginal
septum 2 mm,
with atretic vagi-
nal
-0.5 cm x 1.3 cm x 4.4 cm
with
hematotrachelos, hema-
tometra
and hematosalphinx
|
Laparoscopic assisted
vaginoplasty
Insertion
of modified corrugated stent
which was
removed after
1 month.
|
16 months follow up - return
of regu-
lar menses
|
Second op- Laparoscopic
assisted re-cannulation
of
transverse vaginal
septum
Insertion of
malecot catheter
|
Prior to her definitive
surgery, vaginal
length
was about 2-3 cm
|
| 2 |
11 years old
|
Vaginal dysgenesis
with
transverse
vaginal
septum-
20 mm
|
MRI transverse vaginal
septum
(0.9x1.3x0.2 cm)
hematotra-
chelos,
hematometra.
|
Laparoscopic drainage of
hematometra and medi-
cal
suppression of menses to
relieve her symptom.
Over
5 months, the blind ended
vagina was dilated
using
hegar dilator size 12-13
given adequate An-
aesthesia
|
Prior to her definitive
surgery, vaginal
length
was about 2-3 cm
|
Laparoscopic assisted
vaginoplasty.
Insertion
of modified corrugated stent
and malekot
catheter
|
Modified corrugated stent
was re-
moved 2 weeks
post operation.
Malekot
catheter was removed 7
months
later 10 months follow up
with
regular self vaginal
dilation -re-
turn of
normal menses
|
| 3 |
14 years old |
Mid transverse vagi-
nal
septum- 20 mm
thickness
Vaginal
length was 5 cm
|
MRI with intravaginal gel-
he-
matometrocolpos due
to lower
transverse
vaginal septum
measuring
1.2 mm thickness.
Distance
between transverse
vaginal
septum and introitus
is
2.2 cm.
|
Laparoscopic assisted
vaginoplasty
Insertion
of modified corrugated stent
and malecot
catheter
|
8 months follow up - return
of normal
regular
menses
Malecot catheter
was removed
with self
vaginal dilation
|
| 4 |
14 years old
|
Mid Transverse Vagi-
nal
Septum
|
CT scan-distended uterine
and
cervical canal
consistent with
imperforate
hymen
|
Examination under
anaesthesia; incision at
imper-
forate hymen
which drained 30 ml blood
and he-
matocolpos
aspiration about 300 ml
blood
|
Re-accumulation of
hematometra
and
hematocolpos 1 month post
op-
eration
|
Transabdominal ultrasound
scan-Hematometra,
hemato-
colpos
|
Laparoscopic assisted
vaginoplasty.
Insertion
of modified corrugated stent
and malecot
catheter
|
Modified corrugated stent
was dis-
lodged 2 weeks
post operatively.
Malecot
catheter was planned for
removal
once patient ready for
self
vaginal dilation
|
| 5 |
10 years old |
Mid transverse vagi-
nal
septum- 10 mm
thickness
Vaginal
length was 4 cm
|
MRI - mid transverse
vaginal
septum 5 mm
thickness located
3.8
cm from the introitus
Hematometra
and
hematocolpos
|
Laparoscopic assisted
vaginoplasty
Insertion
of modified corrugated stent
and malecot
catheter
|
7 months follow up - return
of normal
regular
menses
Malecot catheter
was planned for
removal
once patient is ready for
self
vaginal dilation
|
Discussion
The prevalence of Mullerian Defects is complicated by differences in population, diagnostic technique and an incomplete
classification system which is still being revised to enhance effective communication and to improve clinical care (ASRM MAC
2021). Transverse vaginal septum occurs in approximately 1 in
30,000 to 80,000 women [1,2]. The position of the septum is
generally described as low, mid, or high, though there is no accepted system for classifying the location and a variety of measurements are used in literature. Williams et all in their case series, classified the septum as low if less than 3 cm, mid position
if between 3 and 6 cm, and high if greater than 6 cm from the
introitus [3]. Hematometra, hematosalphinx and endometriosis
can be present, with the incidence of endometriosis greatest
for high septa.
Transverse vaginal septa (<1 cm in thickness) may be treated
with a simple end to end anastomosis of the vaginal epithelium or a Z-plasty [1] aiming to cover all the raw surfaces. In our
cases, a modified corrugated stent using the endotracheal tube
connector (Figure 1) was placed post operatively in the vagina
in addition to Z-plasty method to help in promoting epithelization. The concept on its corrugated or rugae like feature can
help in preventing any ingrowth of vaginal tissue preventing
peri-fibrotic tissue adhesion around the stent that ease the removal of the stent post-operatively. The removal can be easily
done in outpatient clinic. It is cost effective and light in weight.
In summary, the modified stent was scheduled for removal in 2
to 4 weeks post surgery. Out of the 5 cases, one was dislodged
in less than 2 weeks, two patients felt discomfort while they
were in sitting position and one patient complained of vaginal
pain. Patients did not develop infection with no evidence of fever or per vaginal foul-smelling discharge. Menstrual flow continued through the lumen of the stent.
In cases of re-stenosis (1/5), high transverse vaginal septum
and patient immaturity in handling post-operative vaginal dilation, malecot catheter was inserted. Malecot 4 wing catheter
is known to be used as drainage catheter following open renal
or bladder surgeries. Malecot wings or mushroom- tip are employed to provide enhanced drainage and promote catheter
retention. It provides maximum softness for enhanced patient
comfort. In 2 out of 5 cases, the catheter was removed easily
in clinic, the patients did not complain of any pain with movement and there was no evidence of infection. In addition, the
catheter can serve as a guide for future vaginal dilation when
young patient reached was ready. The challenges that were encountered includes fibrotic growth around the catheter after 6
months, where separation was done under general anaesthesia. Initiation of vaginal dilation will need adequate analgesia to
reduce the patient’s long term psychological impact.
Laparoscopy assisted vaginoplasty is useful for resection of
high septa. It facilitates resection of the septum and reduces
the surgical related complication. This novel laparoscopic approach to management of high transverse septa was introduced
by William et al. 2013 [4]. In our experiences, a thick septa and
partial vaginal agenesis can be managed in a similar manner.
In our series, intra-operatively, no surgical complications were
encountered with operative surgical time ranging between 60
to 90 minutes. The estimated blood loss is about 50 to 100 mls.
If menstruation can be medically suppressed, some surgeons
advocate daily dilation of the lower vagina for several months
in order to increase vaginal length and to decrease the distance
that will require bridging during septum resection which was
described as Frank’s vagina dilation, 1938. In one of the cases of
transverse vaginal septum with atretic vagina, gradual dilation
of the vaginal was performed prior to definitive surgery. This
was used to force the mucous membrane inward into the introital region and no incision was required. Decades after Frank’s
first description, several studies reported favourable outcomes
using his method [5].
Various methods have been described in few case reports
including the use of silicone stent and tracheobronchial stent
[6,7]. Vaginal dilation at this young age can be a great challenge
to the patient. With the progress of Mullerian anomaly surgery
in the last decade, fertility sparing techniques with fewer complications are becoming the target for gynaecologists especially
in this reproductive age group. Throughout our year of practice, the impact that gynaecologists experienced every time a girl presented with re-stenosis was devastating. This was the
first case series described based on our own institutional experience in dealing with transverse vaginal septum, including its
post-operative care and the detailed procedures performed on
our young adolescent girls. The surgical outcomes were encouraging, and all of the girls were pleased with their return of normal life. As indicated by the case series, the surgical approaches
used result in the least surgical complications and surgery time
as well as minimized girls’ psychological impact.
Conclusions
Primary surgery with minimal manipulation and insertion of
modified corrugated drain can help in maintaining the vaginal
patency especially in young patients. In cases of re-stenosis,
high transverse vaginal septum, and patient immaturity in handling post-operative vaginal dilation, malecot catheter insertion
can be one of the additional option.
Declarations
Funding: The research did not receive any funding or grant.
Patient consent: Written informed consent was obtained
from the patient and patient’s parents for the related image
and no personal information or details are included that may
identify the patient.
Author contribution statement: Author 1 is the first author
who collected and analyzed the data, applied for ethical approval and wrote the manuscript. Additionally, she was one of
the gynaecologist who managed the patients. Author 2 is the
principal supervisor who conceived of the notion given. She is
also the primary pediatric and adolescent gynaecologist for all
patients. She created the idea, edited the manuscript and offered ideas for its improvement. In addition, she authorized the
final draft of the manuscript. Author 3 is also the pediatric and
adolescent gynaecologist who involved actively in the management of all patients. She proofread the manuscript and offered
suggestions for its improvement.
Conflict of interest: The authors declare that no conflicts of
interest associated with this publication.
References
- Ridhima Gupta, Joseph D. Bozzay, David L. Williams, Robert T.
DePond, and Pickens A. Gantt, “Management of Recurrent
Stricture Formation after Transverse Vaginal Septum Excision,”
Journal of Case Reports in Obstetrics and Gynecology, Volume
Article ID 975463. 2015.
- Miller R, Breech L. Surgical correction of vaginal anomalies. Clin
Obstet Gynecol. 2008; 51(2): 223-236.
- William CE, Nakhal RS, Hall-Craggs MA, Wood D, Cutner A, Pattison SH, Creighton SM. Transverse vaginal septae: management
and long term outcomes. BJOG. 2014; 121: 1653-9.
- Williams, C.E., Cutner, A.C. & Creighton, S.M. Laparoscopic management of high transverse vaginal septae: a case report. Gynecol Surg. 2013; 10: 189-191 (). https://doi.org/10.1007/s10397-
013-0799-z.
- Stephen Robson, Gillain D Oliver Management of vaginal agenesis: review of 10 years practice at a tertiary referral centre. 2008.
- Qin Chenglu, Du Min, Zhang Ke, et al. Luohu III Operation for
Congenital Cervical and Vaginal Atresia: Case Report. Chin J
Min Inv Surg. 2016; 16(1). https://doi:10.3969/j.issn.1009-
6604.2016.01.021.
- Novel use of tracheobronchial stents in cervical stenosis and
Mullerian anomalies. S. N. Babayev, B. Reed, E.E. Wilson. OB/
GYN, UT Southwestern Medical Center, Dallas. 2015.