Introduction
For lack of structural continuity on the maxillary dentoalveolar process and the palate region, dentoalveolar aberrations of
the maxillary arch with different severities on the cleft and non-cleft sides are a well-recognized feature characterizing repaired
complete unilateral clefts of the lip and palate (UCLP) patients.
Especially, in the vicinity of the alveolar clefts, it is pointed out
that teeth malposition such as rotation or displacement is characteristically manifested [1-18]. It is said that several explanations have been given as to the dentition dimensional aberration causes, including surgical interference or the primary tissue
deficiency in the congenital clefts [10].
With regard to the teeth malposition in the vicinity of the
alveolar clefts, it is reported that the cleft side permanent maxillary central incisor, which was the terminal tooth in the greater
hemimaxilloalvolar segment, was distally inclined toward the
cleft with high frequency [19,20], and that there was a great
chance of palatal inclination or displacement of the cleft side
permanent maxillary canine along with supporting alveolar process [10]. In these published literatures, it is interesting to note
that there seem the different teeth malposition patterns in the
vicinity of the alveolar clefts, based on whether the tooth is in
the greater hemimaxilloalvolar segment or the lessor hemimaxilloalveolar segment.
To solve those teeth malposition problems caused by cleft alveolar, comprehensive orthodontic treatment following surgical
therapy for maxillary and alveolar cleft, including the secondary alveolar bone graft surgery [21,22], has been performed.
Hence, in order to enhance the clinical judgment and improve
treatment outcomes for the alveolar cleft, it would be desirable
if we could collect, recognize, and better understand valid information of the intrinsic features of the alveolar process in the
vicinity of the alveolar clefts.
For the morphological analysis of the dentoalveolar region
in clefts the lip and palate patients, it is said that the dental cast
has significant advantage of an entity possible to carefully observe and evaluate in terms of study materials [8]. Furthermore,
valid information could be provided objectively and quantitatively, from processing that can be carried out on the digital
data obtained from the whole surfaces of the dental cast only,
that is, a single information source [23].
The aim of the current study was to determine the patterns
and magnitudes of the aberrations in dentoalveolar structure
in the vicinity of the clefts prior to surgical therapy for maxillary
and alveolar clefts, by retrospectively comparing the differences in the morphology of the maxillary alveolar process between
the cleft and non-cleft sides in the 12 children with unilateral
cleft lip and palate in the deciduous dentition to examine morphological features of alveolar process.
Patients and methods
Following Research Ethics Board approval, 7 Japanese girls
and 5 Japanese boys with right unilateral cleft lip and palate
were examined. They were surgically treated by the Millard
technique at the ages of 6 months at Hokkaido University Hospital Plastic Surgery Department, Japan, by any of the department’s five staff surgeons, and the push-back procedure which accompanied posterior shifting of palatal flap at the ages of 18
months by one surgeon (Motonori Kudo) at Oral Surgery Department of the same hospital. None of them had undergone
surgical therapy for maxillary and alveolar clefts, and any orthodontic treatment.
Maxillary dental casts were used for exploration their morphological features of alveolar process in the vicinity of the cleft.
The mean age of the children in the current study at which the
casts had been taken was 6.5 years (range: 6.0-6.9 years) in the
deciduous dentition stage (Hellman’s dental age IIC), and the
cleft side deciduous lateral incisors of all of them were absent,
that is, the cleft side deciduous maxillary central incisors were
the terminal teeth in the greater hemimaxilloalvolar segment
and the cleft side deciduous maxillary canines were the terminal teeth in the lessor hemimaxilloalvolar segment.
The whole surface of the maxillary dental cast was measured
by the optical measurement apparatus which we had developed [24-26]. This apparatus employs a 0.6 mW He-Ne laser
and a 2048-element CCD line image sensor optical system. An
X-Y table and reflection mirrors were used for scanning. The
depth of measurement points on the cast surface was determined by the triangular method, with an accuracy of 0.02 mm.
Scanning pitch was adjusted to the minimum level of the apparatus, which was 0.24 mm in the current study.
The maxillary dental casts were mounted on the X-Y table,
which was referred to as the horizontal reference plane for the
maxillary alveolar structures analysis, with their occlusal planes
parallel to the table. The occlusal plane was constructed by
three points on the teeth, the mesioincisal edges of the cleft
side deciduous maxillary central incisor and the mesiolingual
cusp tips of the right and left second deciduous maxillary molars.
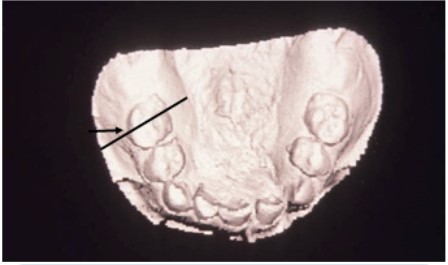
Figure 1 shows an image of the maxillary dental cast obtained from the one child of the 12 children. 157,500 points
were recorded from the maxillary cast surface. The two points,
that is, the apical base point and the crest point of the alveolar
process, used for the maxillary alveolar structures analysis were
determined on a sagittally sectioned image passing through
the midpoint of the mesiodistal anatomic crown width of an
erupted tooth of the dental cast surface for identification on a
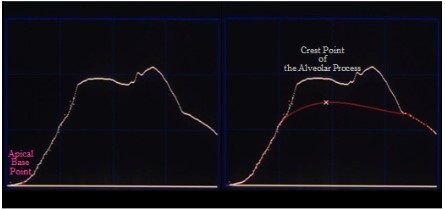
computer display (Figure 1 (a straight arrow)). As shown Figure
2 (left), the apical base point defined as the deepest point on labial or buccal contour of the alveolar process and oral vestibule.
As shown in Figure 2 (right), the crest point was determined as
follows: on a sagittally sectioned image of the dental cast surface, the tooth was disregarded and the midportion of the ridge
was interpolated by the spline function [27]. Next, the most
prominent point of the ridge was established as the crest point.
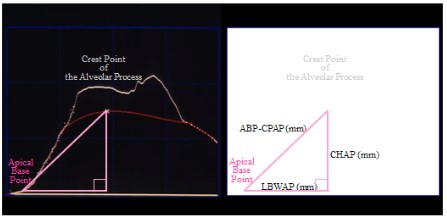
Figure 3 shows the measurements of the maxillary dental
casts used in the current study. Three linear variables were
measured.
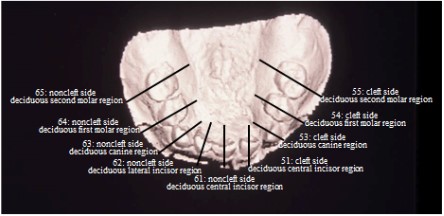
As shown in Figure 4, on the noncleft side, the maxillary dental cast was measured: 61, at the deciduous central incisor; 62,
at the deciduous lateral incisor; 63, at the deciduous canine; 64,
at the deciduous first molar; 65, at the deciduous second molar,
and on the cleft side, it was measured: 51, at the deciduous
central incisor; 53, at the deciduous canine; 54, at the deciduous first molar; 55, at the deciduous second molar.
Paired t-tests were used to compare the differences in morphology of maxillary alveolar process between the cleft and
non-cleft sides using paired measurements from only those
maxillary dental casts. P<.05 was considered statistically significant. For statistical analysis, the SPSS statistical program v14.0
(SPSS Inc, Chicago, IL) was used.
Results
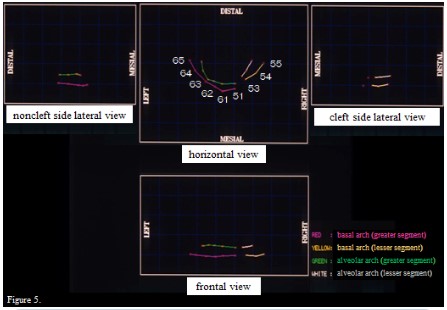
Figure 5 shows the mean plots of the basal arch and the alveolar arch of the 12 children. The basal arch (illustrated in red for
the greater hemimaxilloalveolar segment and in yellow for the
lesser hemimaxilloalveolar segment) was constructed using the
apical base points and the alveolar arch (illustrated in green for
the greater hemimaxilloalveolar segment and in white for the
lesser hemimaxilloalveolar segment) was drawn by connecting
points on the crest of the alveolar process. From horizontal view
projected to the horizontal reference plane, noncleft side lateral
view, cleft side lateral view, and frontal view, respectively, morphological features in visual impression were examined. From
the horizontal view: overall, the alveolar arch was palatally seen
relative to the basal arch; in the deciduous central incisor region, the crest of the alveolar process on the cleft side deviated
labially when compared with the noncleft side; whereas, in the
deciduous canine region, that on the cleft side deviated palatally. From the lateral views and the frontal view: in the deciduous
both central incisor and canine regions, the crest height of the
alveolar from the apical base point was lower on the cleft side
than on the noncleft side.
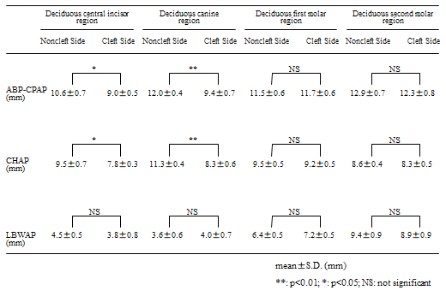
Table 1 gives a comparison of alveolar process morphology
on the cleft side vs the noncleft side. In the deciduous central
incisor and canine regions, distance between the apical base
point and the crest point of the alveolar process (ABP-CPAP)
on the cleft side were significantly smaller than on the noncleft
side (p<0.05 in the deciduous central incisor regions, p<0.01 in
the deciduous canine regions) and height to the crest point of
the alveolar process from the apical base point (CHAP) on the
cleft side were also significantly smaller than on the noncleft
side (p<0.05 in the deciduous central incisor regions, p<0.01
in the deciduous canine regions). As to horizontal distance between the apical base point and the crest point of the alveolar
process (LBWAP) in the deciduous central incisor regions, no
significant difference was found in the comparison between the
cleft side and the noncleft side; however, that on the cleft side
showed a small but definite reduction than on the noncleft side; while, in the deciduous canine regions, no significant difference
was found in the comparison between the cleft side and the
noncleft side; however, that on the cleft side showed a small
but definite increase than on the noncleft side. In the deciduous
first and second molar regions, there were no clear differences
between the alveolar process morphology of the 2 sides in the
current study.
Table 1: Comparison of alveolar process morphology on the
cleft side vs the non cleft side.
Discussion
The current study focused on outcomes of maxillary alveolar
process morphology as a result of primary lip repair in UCLP
children with unrepaired maxillary and alveolar clefts. To measure maxillary alveolar process morphology in detail, we used
the whole surface of the maxillary dental cast. Thus, we could
conduct the study to obtain the reliable and intriguing findings
from a single information source.
The conception of the apical base, which is foundation for
analysis of alveolar process morphology, was originated with
the apical base theory proposed by Lundström [28-33]; the apical base would in the horizontal plane coincide with the region
in which the apices of the teeth roots were located. Therefore,
the apical base should be anatomically defined including bony
substance immediately surrounding the apices of the teeth
roots. In orthodontic practice, based on the apical base theory
[28-33], using the deepest point on labial or buccal contour of
the alveolar process and oral vestibule, which is regarded as an
immediate surrounding region of the apices of the teeth roots,
the basal arch width and length were measured on the plaster model analysis [34]. In this regard, we believe it appropriate
that we determined the apical base point: point defined as the
deepest point on labial or buccal contour of the alveolar process and oral vestibule, and analyze morphology of the alveolar
process based on the line passing through the point in the current study.
In the current study, both distance between the apical base
point and the crest point of the alveolar process (ABP-CPAP) and
the crest height of the alveolar process (CHAP) in the cleft side
deciduous both central incisor and canine regions, that is, at the
distal terminal end of the greater hemimaxilloalveolus and the
medial terminal end of the lesser hemimaxilloalveolus, were
significantly smaller than in the noncleft side that regions; in
accordance [35,36], these findings suggest that the presence of
maxillary and alveolar cleft itself substantially restricts the vertical size of the alveolar process in unilateral cleft lip and palate
children. Explained that the reduction in vertical development
was ascribed to the cleft malformation [20]. Paulin pointed out
that the aberration of the alveolar process would give insufficient bony support to the teeth in the cleft region for eruption in their correct position [37]. It is reported, as mentioned
above, that there seem characteristic teeth malposition in the
vicinity of the alveolar cleft with high frequency in clefts the lip
and palate patients; suspected that the particular morphologic
aspect of alveolar cleft itself is a factor involving the malposition
[10,18]. We assume, therefore, that inadequate vertical growth
of the alveolar process in the vicinity of the alveolar cleft, as
seen in the current study, accompanied with the characteristic
teeth malposition, would be attributed to the intrinsic effects of
congenital alveolar cleft itself, apprehended to cause the characteristic teeth malposition in the stage of permanent dentition, which is another subject we must deal with in the future.
As to horizontal distance between the apical base point and
the crest point of the alveolar process (LBWAP), in the current study, we observed in the comparison between the cleft
side and the noncleft side that the crest of the alveolar process in the vicinity of the cleft at the distal terminal end of the
greater hemimaxilloalveolus deviated labially; conversely, that
at the medial terminal end of the lesser hemimaxilloalveolus
deviated palatally. From these findings, it seems reasonable to
assume that the patterns of the labiopalatal inclination of the
alveolar process in the vicinity of the cleft are probably different
between at the distal terminal end of the greater hemimaxilloalveolus and the medial terminal end of the lesser hemimaxilloalveolus.
Determined the local deformation (strain) of the upper lip
using ultrasound elastography in unilateral cleft lip and palate
patient that underwent a surgical reconstruction of a unilateral
cleft lip [38], and revealed asymmetric muscular strain between
on the cleft side and the noncleft side, with greater strain on
the noncleft side. Furthermore, noted the influence of asymmetric muscular contraction and pull on the alveolar process
toward the noncleft side and suggested that the asymmetric
muscular strain should be one of the factors that could influence maxillary dentoalveolar formation in cleft lip and palate
patients [18]. Considering these views, we assume that the effects of muscular function are among the most important factors involved in our finding, that is, the pattern differences of
the labiopalatal inclination of the alveolar process in the vicinity
of the cleft between between at the distal terminal end of the
greater hemimaxilloalveolus and the medial terminal end of the
lesser hemimaxilloalveolus.
In contrast, in the deciduous first and second molar regions,
there were no clear differences between the alveolar process
morphology of the cleft side and the noncleft side in the current
study. Therefore, we are confident that we could determine the
morphological features of alveolar process in the vicinity of the
cleft prior to surgical therapy for maxillary and alveolar clefts
in the deciduous dentition in unilateral cleft lip and palate children.
We hope that the findings of our current study would be
useful information for those specializing in treating cleft palate
patients, in establishing a guideline on treatment planning for
optimal orthodontics or surgical treatment and its appropriate
time, and in qualitatively improving the treatments.
Conclusion
(1) The current study suggests that the presence of maxillary
and alveolar cleft itself substantially restricts the vertical size of
the alveolar process in the vicinity of cleft in unilateral cleft lip
and palate child.
(2) In the current study, it seems reasonable to assume that
the patterns of the labiopalatal inclination of the alveolar process in the vicinity of the cleft are probably different between
at the distal terminal end of the greater hemimaxilloalveolus
and the medial terminal end of the lesser hemimaxilloalveolus.
Declarations
Acknowledgements: The authors gratefully acknowledge
the statistical suggestion of Dr Masahiro Mizuta, DEng, who is
the Professor of Theoretical Information Science Laboratory,
Center for Information and Multimedia Studies, Hokkaido University.
The authors have no conflict of interest to disclose.
Funding: Not applicable.
References
- Hagerty RF, Andrews EB, Hill MJ, Calcote CE, Karesh SH, et al.
Dental arch collapse in cleft palate. Angle Orthod. 1964; 34(1);
25-36.
- Pruzansky S, Aduss H. Arch form and the deciduous occlusion in
complete unilateral clefts. Cleft Palate J. 1964; 1(4); 411-418.
- Huddart AG, Orth D. Maxillary arch dimensions in bilateral cleft
lip and palate subjects. Cleft Palate J. 1970; 7(1); 139-155.
- Wada K. Growth changes in dimensions and form of the maxillary arch in complete unilateral cleft lip and palate infants. J
Osaka Univ Dent Soc .1972; 17(2): 81-101.
- Abe M. A study on chronological changes of the upper dental
arch in cases of unilateral cleft lip and palate after labioplasty.
Jpn J Oral Maxillofac Surg. 1974; 20(3): 248-267.
- Hirose T. A study on chronological changes of the upper dental
arch in cases of isolated cleft palate after palatoplasty. J Jpn Cleft
Palate Assoc. 1979; 4(1): 15-47.
- Mizokawa N. Tri-dimensional maxillary growth, from infancy to
4 years of age, of patients-with cleft palate according to their
cleft types. J Jpn Cleft Palate Assoc. 1982; 7(1): 1-20.
- Genba R, Komatsu Y. Clinical studies on the morphology of the
dental arch and palate in children with cleft lip and palate. J Jpn
Cleft Palate Assoc. 1983; 8(1): 67-84.
- Shinjo N, Takizawa Y, Shibasaki Y, Fukuhara T. A study of maxillary
segmental collapse in children with unlateral cleft lip and palate:
Arch form and occlusal aberration. J Showa Univ Dent Soc. 1991;
11(2): 242-254.
- Šmahel Z, Tomanová M, Müllerová Z. Position of upper permanent central incisors prior to eruption in unilateral cleft lip and
palate. Cleft Palate Craniofac. J. 1996; 33(3): 219-224.
- Aso M. Observations of postoperative changes in the dental
arch in unilareral cleft lip and palate patients. Jpn J Oral Maxillofac Surg. 1996; 42(4): 387-395.
- Tortra C, Meazzini MC, Garattini G, Brusati R. Prevalence of abnormalities in dental structure position, and eruption pattern in
a population of unilateral and bilateral cleft lip and palate patients. Cleft Palate Craniofac J. 2008; 45(2): 154-162.
- Lai MC, King NM, Wong HM. Abnormalities of maxillary anterior
teeth in Chinese children with cleft lip and palate. Cleft Palate
Craniofac J. 2009; 46(1): 58-64.
- Pegelow M, Alqadi N, Karsten AL. The prevalence of various dental characteristics in the primary and mixed dentition in patients
born with non-syndromic unilateral cleft lip and palate. Eur J Orthod. 2012; 34(5): 561-570.
- Jabbari F, Skoog V, Reiser E, Hakelius M, Nowinski DD. Optimization of dental status improves long-term outcome after alveolar
bone grafting in unilateral cleft lip and palate. Cleft Palate Craniofac J. 2015; 52(2): 210-218.
- Disthaporn S, Suri S, Ross B, Tompsonb B, Baenaf D, et al. Incisor
and molar overjet, arch contraction, and molar relationship in
the mixed dentition in repaired complete unilateral cleft lip and
palate: A qualitative and quantitative appraisal. Angle Orthod.
2017; 87(4): 603-609.
- Rark YH, Park S, Baek SH. Alignment strategy for constricted
maxillary dental arch in patents with unilateral cleft lip and palate using fixed orthodontic appliance. J Craniofac Surg. 2018;
29(2): 264-269.
- Suri S, Disthaporn S, Ross B, Tompsonb B, Baenaf D, et al. Permanent maxillary central incisor and first molar rotations in the
mixed dentition in repaired unilateral cleft lip and palate and
their relationship with absence of teeth in their vicinity. Angle
Orthod. 2018; 88(5): 567-574.
- Ohyama K, Motohashi N, Kurod T. Abnormalities of the teeth adjacent to a cleft and their orthodontic management. J Jpn Cleft
Palate Assoc. 1981; 6(2): 40-49.
- Nakagawa H, Tanne K, Ohyama Y, Maeda S, Ohmae H, et al. Investigation on anomalies of teeth and occlusion of the children
with cleft lip and palate. J Jpn Cleft Palate Assoc. 1982; 7(2): 155-171.
- Kochi S. Surgical therapy for maxillary and alveolar cleft in cleft
palate patients: Autogenous particulate marrow and cancellous
bone grafting. Tohoku Univ Dent J. 1998; 17(2): 122-142.
- Kochi S. Clinical and statistical study of surgical therapy for maxillary and alveolar clefts. Tohoku Univ Dent J. 1999; 18(1): 90-94.
- Zilberman O, Huggare JV, Parikakis KA. Evaluation of the validity
of tooth size and arch width measurements using conventional
and three-dimentional virtual orthodontic models. Angle Orthod. 2003; 73(3): 301-306.
- Yamamoto K, Toshimitsu A, Mikami T, Hayashi S, Harada R, et al.
Optical Measurement of dental cast profile and application to
analysis of three-dimensional tooth movement in orthodontics.
Front Med Biol Eng. 1988; 1(2): 119-130.
- Yamamoto K, Hayashi S, Nishikawa H, Nakamura S, Mikami T.
Measurements of dental cast profile and three-dimensional
tooth movement during orthodontic treatment. IEEE Trans
Biomed Eng. 1991; 38(4): 360-365.
- Tomochika A, Ishikawa H, Nakamura S. Development of the
three −dimensional analyzing system for dentoalveolar region
using the system for the shape measurement of dental cast. J
Jpn Orthod Soc. 1995; 54(4): 264-273.
- Rogers DH, Adams JA. Mathematical elements for computer
graphics. New York, 1976, McGraw-Hill. 116-156.
- Lundström AF. Malocclusion of the teeth regarded as a problem
in connection with the apical base. Int Orthod Oral Surg Radiogr.
1925; 11(7): 591-602.
- Lundström AF. Malocclusion of the teeth regarded as a problem
in connection with the apical base. Int Orthod Oral Surg Radiogr.
1925; 11(8): 724-731.
- Lundström AF. Malocclusion of the teeth regarded as a problem
in connection with the apical base. Int Orthod Oral Surg Radiogr.
1925; 11(9): 793-812.
- Lundström AF. Malocclusion of the teeth regarded as a problem
in connection with the apical base. Int Orthod Oral Surg Radiogr.
1925; 11(10): 933-941.
- Lundström AF. Malocclusion of the teeth regarded as a problem
in connection with the apical base. Int Orthod Oral Surg Radiogr
1925; 11(11): 1022-1042
- Lundström AF. Malocclusion of the teeth regarded as a problem
in connection with the apical base. Int Orthod Oral Surg Radiogr.
1925; 11(12): 1109-1133.
- Otsubo J. A study on the tooth material in Japanese adults of
normal occlusion, its relationship to coronal and basal arches. J
Jpn Orthod Soc. 1957; 16(1): 36-46.
- Boyne P, Sands NR. Secondary bone grafting of residual alveolar
and palate. J Oral Surg 1972; 30(2): 87-92
- Crabb JJ, Foster TD. Growth defects in unrepaired unilateral cleft
lip and palate. Oral Surg Oral Med Oral Pathol. 1977; 44(3): 329-335.
- Paulin G, Åstrand P, Rosenquist JB, Bartholdson L. Intermediate
bone grafting of alveolar Clefts. J Craniomaxillofac Surg. 1988;
16: 2-7.
- de Korte CL, van Hees N, Lopata RGP, Weijers G, Katsaros C, et al.
Quantitative assessment of oral orbicular muscle deformation
after cleft lip reconstruction: an ultrasound elastography study.
IEEE Trans Med Imaging. 2009; 28(8): 1217-1222.