Short Commentary
Fetal Electrocardiograph (ST-Analyser or STAN): Is it time for the Requiem?
Edwin Chandraharan*
Director, Global Academy of Medical Education & Training, London, UK.
Director, Global Academy of Medical Education & Training, London, UK.
*Corresponding Author: Edwin Chandraharan
Director, Global Academy of Medical Education & Training, London, UK.
Email: edwin.c@sky.com
Received: Jun 28, 2023
Accepted: Jul 17, 2023
Published: Jul 24, 2023
Archived: www.jclinmedsurgery.com
Copyright: © Chandraharan E (2023).
Cardiotocograph (CTG) was introduced into clinical practice to timely recognise features of the onset of decompensation so that timely action could be taken to avoid hypoxic- ischaemic encephalopathy (HIE) or perinatal deaths. Unfortunately, systematic reviews have shown that classification of CTG traces into “normal, suspicious and pathological” (or “Category I, II and III in the USA) has not only failed to reduce intrapartum operative interventions, cerebral palsy and perinatal deaths, but it was also associated with significant inter- and interobserver variability. Fetal electrocardiograph (ECG) or ST-analysis (STAN) was introduced into clinical practice to reduce the false positive rate of cardiotocograph (CTG) and to reduce the rate of unnecessary intrapartum operative interventions such as emergency caesarean sections, vacuum and forceps births. Although the STAN technology is based on sound physiological principles, its Achilles’ Heel is the continued use of the CTG classification tool using “normal, intermediary and abnormal” by arbitrarily grouping several features into different categories without any robust scientific evidence. This exposes the STAN technology to the same flaws of “pattern-recognition” and inter-and intra-observer variability. In the light of recent systematic reviews and meta-analysis showing no benefit in reducing emergency caesarean section and the most recent randomised controlled trial from Australia suggesting that introduction of STAN technology as an adjunct to CTG has failed to show any reduction in intrapartum operative interventions, frontline clinicians have to ask the question: Is it time for the Requiem for STAN?
Citation: Chandraharan E. Fetal Electrocardiograph (ST-Analyser or STAN): Is it time for the Requiem?. J Clin Med Surgery. 2023; 3(2): 1111.
Fetal ECG (ST-analyser or STAN) was introduced into clinical practice to reduce the false positive rate of “Pathological”, “Abnormal” or “Category III” CTG traces to avoid the over-reaction to patterns by frontline clinicians. This is because it has been shown that the vast majority of CTG traces are not associated with fetal acidosis [1-5], and recent systematic reviews have shown that CTG does not reduce the likelihood of cerebral palsy and perinatal deaths but has increased the likelihood of emergency caesarean sections and operative vaginal births [6]. Moreover, recognition of various patterns in isolation and then grouping them into different “categories” have been fraught with human errors of “pattern-recognition” resulting in inter and intra-observer variability [7-9]. Even those who consider themselves as “experts” in CTG interpretation have been reported to change their own CTG classification retrospectively when they are made aware of the neonatal outcomes [10,11]. As a “knee-jerk” reaction to increasing emergency caesarean section rates as a result of introducing CTG into clinical practice without any robust Randomised Controlled Trials (RCT), additional tests (also called adjunctive technology) such as fetal pulse oximetry and Fetal Scalp Blood Sampling (FBS) were introduced into clinical practice in the hope of reducing emergency intrapartum operative interventions by reducing the false positive rate of the CTG. These “additional” tests have failed to live up to the expectations of those who introduced them into clinical practice because systematic reviews have shown that both fetal pulse oximetry [12] and fetal scalp blood sampling using scalp pH [6], and lactate [13] do not reduce intrapartum operative interventions. On the contrary, recent evidence have shown that FBS may increase the caesarean section rate [14,15], which should not be surprising to any frontline clinician who understands the very basic human physiology. In hypoxic stress, it is well known that the human compensatory response is to release catecholamines to cause peripheral vasoconstriction to centralise blood flow from the skin. This would make the skin, which is a peripheral “non-essential” tissue during hypoxic stress, to undergo anaerobic metabolism leading to the production of lactate. Therefore, if a sample of capillary blood is taken from the skin of the fetal scalp, obviously it would be acidotic, reflecting the normal compensatory physiological response (i.e., catecholamine mediated vasoconstriction to re-distribute blood flow to central organs) to ongoing stress [16]. Misclassifying excess of lactate in the skin due to this normal physiological compensation as “abnormal” would lead to increased intrapartum operative interventions. Therefore, the role of FBS in contemporary obstetric practice has been questioned [17-19]. In fact, FBS was not performed in the USA in routine clinical practice for more than 20 years, and more recently, the National Institute of Health and Clinical Excellence (NICE) in the UK has also stopped recommending FBS due to lack of scientific evidence that FBS reduces the false positive rate of CTG [20].
Fetal ECG (St-analyser or STAN) was introduced into clinical practice as an additional test of fetal wellbeing to reduce the false positive rate of CTG by continuously analysing the fetal central organ (myocardium) during labour. Although initial RCTs had shown evidence of benefit in reducing operative interventions [21,22], a subsequent large RCT [23] and meta-analysis of systematic reviews [24] have failed to show any benefit of STAN in reducing emergency caesarean sections. More recently, a large observational study from Norway suggested that STAN may increase the number of babies with low Apgar scores without reducing intrapartum operative interventions [25]. Therefore, it is only fair that all right-minded and right-thinking frontline clinicians who are focussed on practising evidence-based medicine should ask the question “should STAN be discontinued from clinical practice, and suffer the same fate as fellow adjunctive technologies such as fetal pulse oximetry and FBS?’.
What is the physiological principle behind the STAN Technology?
Myocardium has a positive energy balance when the oxygen supply through the coronary blood vessels is greater than the demand due to the ongoing cardiac workload. This aerobic metabolism generates a total of 38 Adenosine Triphosphate Molecules (ATPs) which is utilised by myocardial cells to ensure optimum myocardial contractility to maintain the required cardiac output necessary to meet the metabolic requirements of the myocardium, the brain and all other fetal organs. At the onset of recording, the STAN computer calculates the ratio of the height of the T wave (reflects ventricular repolarisation and relaxation) and the QRS complex (reflects ventricular depolarisation and contraction), which is usually approximately below 0.25 because of the smaller size of the “T-wave” as compared to the larger “QRS complex”. Moreover, the STAN computer also analyses the morphology of the ST segment because if the myocardial energy balance and electrical conduction are both normal, then the ST segment will be stable and remain “isoelectric”. If there is insufficient oxygen to meet the metabolic requirements of the myocardium, then, the resulting negative myocardial energy balance would trigger an anaerobic metabolism within the myocardium. The release of catecholamines to ensure immediate vasoconstriction of the peripheral blood vessels to centralise blood flow to the myocardium would also trigger myocardial glycogenolysis through the beta-2 adrenergic receptors. Breakdown of the stored myocardial glycogen to glucose to provide the myocardium with additional energy substrate would increase the intracardiac potassium levels. This myocardial hyperkalaemia causes changes in the fetal electrocardiograph resulting in “tall” or “tented” T waves. If the observed height of the T wave is significantly higher than the initially recorded height of the T wave then, the STAN computer would recognise this as a “significant change” and then will generate a “ST Event”. If the ongoing hypoxic stress which resulted in myocardial glycogenolysis is short lasting (<10 minutes), then, an “Episodic” T/QRS Event will be generated. In a longer lasting hypoxic stress with glycogenolysis (>10 minutes), a “Baseline” T/QRS Event will be generated. If there is a primary myocardial membrane instability (e.g., chorioamnionitis with myocarditis), or an abnormal electrical conduction within the myocardium (cardiomyopathies and cardiac conduction defects) resulting in the ST Segment moving above or below the isoelectric line, then a “Biphasic ST Event” will be generated. Therefore, unlike fetal pulse oximetry and FBS which attempted to detect the oxygenation of a non-essential peripheral tissue (skin) which is compressed in labour (caput and moulding) resulting in erroneous results, the STAN technology continuously analyses a fetal central “high-priority” organ (myocardium) to timely detect the onset of negative myocardial energy balance and resultant catecholamine-mediated myocardial glycogenolysis.
If the STAN Technology is based on sound scientific principles, then, what is the problem?
The “Achilles Heel of STAN” is not the technology, but the tools that have been produced to interpret the significance of the observed STAN Events. Frontline clinicians are expected to classify the CTG trace according to a classification table (Figure 1) which is based on the old FIGO Guidelines of 1987 to determine whether an intervention was required and, if so, the rapidity of that required intervention.
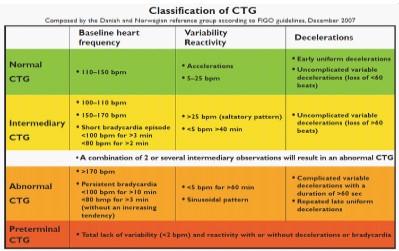
Unfortunately, this table was not based on robust scientific evidence, and is likely to significantly increase inter and intra-observer variability that has plagued CTG interpretation [26,27]. The flaws in the CTG guideline used whilst interpreting STAN Events have been highlighted in Table 1.
| Physiological Principles | Violation of basic Physiological Principles by STAN CTG Guidelines | |
|---|---|---|
| Population-based studies have suggested that the normal baseline FHR is 110-160 bpm | There is no evidence to recommend 110-150 bpm as the normal range Classifying 150-170 bpm as “intermediary” will miss fetuses with chorioamnionitis and growth restriction leading to poor outcomes | |
| Decelerations are cardioprotective reflexes designed to protect the myocardial positive energy balance by rapidly reducing the myocardial workload in response to repetitive and intermittent hypoxic stress | Classifying them by “uncomplicated and complicated” by arbitrary, unscientific cut off for both duration and amplitude is likely to increase intrapartum operative interventions and result in inter and intra-observer variability resulting in poor maternal and perinatal outcomes. | |
| Isolated, decelerations or recurrent decelerations with an intervening stable FHR baseline and reassuring variability have no correlation with poor perinatal outcomes | Decelerations are classified in isolation into “normal, intermediary and abnormal” categories, without any consideration to fetal response to stress increasing the likelihood of operative interventions | |
| “Short Bradycardia Episode” of >3 minutes as an “Intermediary Feature” | This ignores the differentiation between a prolonged deceleration (3-10 minutes) and fetal bradycardia (>10 minutes) as stated by international consensus guidelines on CTG interpretation [28,29]. | |
| Reduced baseline FHR variability without preceding decelerations and / or an increase in the baseline FHR does not reflect fetal hypoxia and acidosis and reflects normal fetal cycling behaviour (alternative epochs of active and deep sleep cycles) | Arbitrary classifying reduced baseline variability for >40 minutes as “intermediary” and >60 minutes, in isolation, as “abnormal” without robust scientific evidence, and without considering the rise in the baseline and ongoing decelerations is likely to increase operative interventions. Conversely, failure to take action for 40 or 60 minutes in the presence of ongoing decelerations and / or a rise in the baseline FHR would significantly increase the likelihood of poor perinatal outcomes. | |
| The erratic increased variability during labour (ZigZag pattern) which occurs due to a rapidly evolving hypoxia is different to the uniform increase in variability (saltatory pattern) which occurs due to an antenatal insult and requires an urgent intervention to reduce hypoxic stress [30,31]. | The guideline simply states that “saltatory pattern” is an intermediary feature without providing any duration to consider this feature as abnormal. Moreover, it disregards the fact that increased variability is a very serious feature during labour, especially if uterotonics are used or during active maternal pushing, and requires an immediate intervention to oxygenate the fetus. | |
| All CTG features do not have the same correlation to poor perinatal outcomes. Morphologically “ugly-looking” decelerations do not indicate fetal compromise. Different types of fetal hypoxia have different sequence and associated CTG features | By blindly stating “a combination of 2 or several intermediary observations will result in an abnormal CTG”, the guideline has completely failed to appreciate the specific features of gradually evolving and subacute hypoxia and specific features of chorioamnionitis which may increase the likelihood of poor perinatal outcomes. |
Is there any evidence that poor knowledge of fetal physiological responses whist using STAN Technology leads to poor perinatal outcomes?
STAN technology was introduced at St George’s Hospital in London in June 2002, and the authors who analysed the first 1502 cases concluded that “In our unit, the introduction of STAN technology has not changed the incidence of emergency operative delivery or NNE. Further strategies to improve our obstetric outcomes are needed. Our experience suggests the need for more intensive training and assessment of the users regarding the use of the CTG and ST analysis, with emphasis on the need to take prompt action when significant ST and CTG changes are present. Better training, assessment and supervision of users may help improve outcome” [32]. Out of these 1502 cases monitored with STAN technology, there were 14 cases of Neonatal Encephalopathy (NNE), and all but one case (i.e., 13 cases) had substandard care relating to delay in taking action, failure to take any action, and lack of knowledge to recognise the features of a preterminal CTG trace. The authors had honestly concluded that “our experience suggests the need for more intense training on interpretation of CTG and strict adherence to guidelines” [32]. Therefore, it has been shown that a lack of training on fetal physiological responses and it appears the use of a guideline which was not based on robust scientific evidence (Figure 1) or on basic physiological principles (Table 1) contributed to these unfortunate poor outcomes. Unfortunately, the same STAN guidelines were also used in Netherlands in cases of chorioamnionitis and fetal sepsis, which unsurprisingly and unfortunately resulted in poor perinatal outcomes [33]. Based on the erroneous guideline not only the clinicians missed higher than expected baseline FHR and the absence of cycling due to the lack of basic fetal physiological knowledge, they had also performed fetal blood sampling in conjunction with STAN [33]. This illogical practice of checking the pH of the fetal skin whilst continuously monitoring the fetal myocardial oxygenation by the STAN technology usually increases the rate of unnecessary operative interventions because of the anaerobic metabolism in the skin due to peripheral vasoconstriction to centralise blood flow as part of normal fetal compensatory responses, being mistaken as “fetal distress”. However, in this case, due to lack of basic physiological knowledge, the clinicians misunderstood normal pH of the fetal scalp due to peripheral vasodilation in fetal infection (i.e., not vasoconstriction) as “absence of distress” leading to disastrous consequences for the fetus and the family. Unfortunately, several STAN “experts” recommended, advocated and also used FBS in their own clinical practice in conjunction with STAN [34], and this very likely blunted the positive benefits of the STAN technology in reducing intrapartum operative interventions.
Is there any evidence that training on fetal physiological responses whist using STAN technology improves maternal and perinatal outcomes?
In view of increased rate of hypoxic-ischaemic encephalopathy (HIE) at St George’s Hospital in London after introduction of the STAN technology without robust training of staff, an external Panel Review took place in 2004, which resulted in the appointment of a new labour ward lead consultant to improve maternal and perinatal outcomes in 2005. The new labour ward lead consultant worked with the multi-disciplinary team and the fetal monitoring midwives to first stop ongoing FBS in conjunction with STAN due to lack of knowledge amongst obstetricians and midwives who used the technology. All staff were trained in physiological interpretation of CTG and on recognising the features of different types of fetal hypoxia, There was an approximately a 50% reduction in intrapartum caesarean sections due to suspected fetal compromise [35]. After the introduction of a mandatory competency assessment on CTG interpretation to confirm the impact of knowledge transfer, there was approximately 50% reduction in the rate of HIE and neonatal acidosis [36,37]. Similar results were reported when STAN Technology was introduced after intense training on fetal physiological responses and a mandatory competency testing in another hospital in Wales.
Need for STAN CTG guidelines based on fetal physiological responses: Proof of the Pudding
The use of STAN/CTG Guidelines with random parameters grouped arbitrarily into “normal, intermediary and abnormal) with continued use of fetal blood sampling with STAN technology at St George’s Hospital in London from 2002 resulted in 13 potentially avoidable cases of HIE in 1502 cases. Therefore, the reported rate of HIE in the group monitored by STAN technology was 8.6/1000 which was significantly higher than the UK National Average (1.5-2.5/1000). The rate of neonatal metabolic acidosis was also high 2.8% [32]. After the introduction of physiological interpretation of CTG and training staff on how to recognise the features of different types of fetal hypoxia and fetal responses to ongoing stress, the rate of neonatal metabolic acidosis was reduced to 0.6% from 2.8%. Moreover, the authors had reported 35 cases of NNE in 14890 births [32]. The overall rate of HIE was 2.3/1000. After the intensive training on fetal physiology, there were only 16 cases of NNE in approximately 52,187 births in the very same hospital [39]. The rate of HIE after intense training on fetal physiological responses and avoiding the error producing STAN CTG Guideline tool and abandoning FBS, was only 0.3/1000. This approximately 8-fold reduction in HIE illustrates the importance of using Physiological Interpretation of CTG whist using STAN technology to maximise its potential.
STAN: A recurrent tale of straws and weeds
The recent Australian STAN Randomised Controlled Trial (START) has concluded that STAN did not reduce the rate of emergency caesarean sections [40]. This will no doubt generate an intense debate from the opponents and proponents of STAN, once again. There will be another series of systematic reviews and meta-analysis with some trying to discredit STAN being confident that this was the last straw that broke the camel’s back, whilst others trying to clutch and grasp the weeds to keep the STAN technology afloat. There will be criticisms on the methodology, number of patients recruited, the power calculation, and that the conclusions are not valid by the supporters of STAN.
The opponents of STAN will simply say “we told you so” and that this is just another RCT confirming the lack of clinical benefit of STAN. In reality both the supporters and opponents haven’t yet grasped the fact that the current CTG tool that was being used by all RCTs, nullifies the true potential of the STAN technology.
Is STAN clinically and scientifically dead requiring a Requiem?
Recently, several authors have been calling for a physiological approach to STAN monitoring to maximise its potential and to reduce the pitfalls of pattern recognition arising from “Normal, Intermediary, Abnormal” [41-43]. One cannot continue to arbitrarily group certain features into different categories and then use FBS to cover the lack of knowledge of fetal physiological responses and not understanding the features of different types of hypoxia whilst using the STAN technology. If the largest US RCT had struck a mortal blow to STAN technology and subsequent meta-analysis and the Norwegian population study had put STAN on the ventilator of evidence-based medicine, the recent Australian STAN RCT is going to reduce the prospects of survival even further, unless urgent action is taken by the manufacturers and those “experts” who had produced the STAN “Normal, Intermediary, Abnormal” Guideline.
After the publication of the first international consensus guidelines on Physiological interpretation of CTG by 34 experts from 14 countries in 2018 [29], there was initial enthusiasm by the manufacturer to change the CTG / STAN Guideline based on Physiological Interpretation of CTG in 2020 which created an initial optimism. (https://www.neoventa.com/2020/11/development-of-clinical-guidelines-based-on-fetal-physiology-forctg-and-st-analysis/).
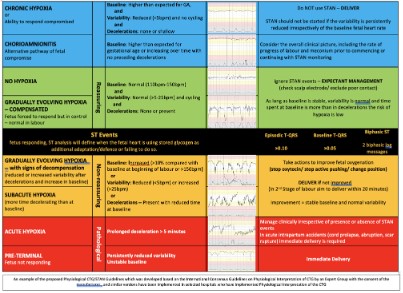
In fact, several hospitals which had introduced Physiological Interpretation of CTG had, quite rightly, refused to use “Normal, Intermediary, Abnormal” when using the STAN technology. This resulted in the development of a physiological CTG/STAN Guideline (Figure 2) which has been implemented in several hospitals across Europe.
However, even three years later, due to apparent lethargy and fear to challenge those who promote “Normal, Intermediary and Abnormal” with the use of FBS, the manufacturer appears to be unable to eliminate the Achilles Heel of STAN, which has resulted in the current predicament of STAN. The loss of the STAN technology due to basic failure to adhere to the principles of fetal physiology whilst interpreting CTG traces to ensure appropriate interpretation of STAN Events will be even a greater loss to women, babies and families. Training STAN users on “physiological CTG interpretation” and then forcing them use a tool that simply groups different FHR features into different categories (Normal, Intermediary and Abnormal) without incorporating the different types of fetal hypoxia and fetal compensatory responses to stress and turning a blind eye to continuing use of FBS in conjunction with STAN is not only illogical but potentially dangerous. This is because this approach would cause confusion amongst frontline clinicians and also would miss babies with chorioamnionitis where the FBS result would most likely be normal due to peripheral vasodilatation. It appears that no lessons have been learnt from the publications from St George’s Hospital in London [32] and Netherlands [33] in 2007 which highlighted that the current CTG / STAN guidelines was ineffective in recognising chorioamnionitis. If the training in physiological interpretation of CTG is to be effective, then the tools to interpret CTG traces whilst using the STAN technology should mirror what is taught during the training. There have been several publications supporting the use of physiological interpretation of CTG [44-54], and therefore, failure to change the CTG STAN interpretation tool to improve maternal and perinatal outcomes cannot be justified in the era of evidence-based clinical practice, founded on sound scientific principles. It has been reported that fetal ECG changes occur in approximately 40% of subacute hypoxia during second stage of labour [55], and therefore, the use of the same CTG interpretation tool with the same parameters without considering the different types of hypoxia, may lead to poor outcomes when the hypoxic stress rapidly evolves during the second stage of labour.
In the author’s opinion, after the publication of the large Norwegian population study in 2022 suggesting increased number of babies with low Apgar scores and the Australian RCT in 2023 suggesting no benefit in reducing emergency caesarean sections, the STAN technology has three potential outcomes. Firstly, based on Einstein’s words of wisdom, if the manufacturer decides to continue printing more and more of the same STAN Interpretation Cards stating “Normal, Intermediary, Abnormal”, then, it is very likely that STAN Technology would die a slow and painful demise and it will face the same fate as other adjunctive technologies. Secondly, if another manufacturer who is focussed on understanding fetal physiological responses, takes over the technology from the current manufacturer and immediately replaces the error producing CTG interpretation tool with physiological interpretation of CTG, then, the STAN technology is likely to survive its “near death experience”. Thirdly, if the current manufacturer develops the courage and conviction to challenge those who had produced this error producing, unscientific classification tool with “Normal, Intermediary, Abnormal” and challenge those who had recommended FBS to mask the lack of knowledge of fetal physiological responses and the features of different types fetal hypoxia, and then they introduce physiological CTG guidelines to complement the STAN technology, to realise it's true potential to improve outcomes for women and babies, then, the STAN technology is very likely to survive its current “near-death experience”. Those of us who have worked with the STAN technology with the incorporation of fetal physiological responses and have seen its true potential to improve maternal and perinatal outcomes can only hope that this technology survives for the sake of women and children. But it cannot do so if the current CTG interpretation tool is continued to be used, and FBS is performed in conjunction with the use of STAN.
The question as to whether the STAN technology requires a Requiem or not entirely depends on how much the current manufacturer and frontline clinicians who use STAN in their daily practice are willing to resurrect it by promoting a physiologi- cal approach to CTG interpretation to maximise its potential.
Conflict of interest: E. C. has been conducting several Master classes on CTG and fetal ECG in the UK, Europe, Asia, and Australia and he was the co-organizer of the Intrapartum Foetal Surveillance Course at the Royal College of Obstetricians and Gynaecologists (RCOG) and Fetal Monitoring Courses at St George’s University of London. He has used fetal ECG (ST-analyser or STAN) for intrapartum fetal heart rate monitoring for over 15 years and was a member of the Editorial Board for NHS e-learning on CTG. He was the Course lead for the Baby Lifeline CTG Masterclasses, and Neoventa CTG and Fetal ECG Master-classes. Organisers of some of these Masterclasses have received sponsorships from Philips, Neoventa, Euroking, Huntleigh, K2 and other industry to support these Masterclasses. However, E.C. does not have any financial or managerial interests in any of these companies. EC was one of the three-member guideline development group which revised the international FIGO Guidelines on CTG in 2015 and was on the Editorial Board of the Consensus Panel which produced the international consensus guidelines on Physiological interpretation od CTG, and he was on the European Expert Group for the development of Physiological CTG/STAN Guideline led by Dr Susana Pereira.