Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 3
Open Access
Volume 3
Greco Cosimo Angelo 1*; Paraninfi Aurora 2; Mangia Federica1; Garzya Massimiliano3; Cucurachi Marco4; Zaccaria Salvatore1
*Corresponding Author: Cosimo Angelo Greco
Cardiac Surgery Department, Vito Fazzi Hospital, Lecce, Italy.
Email: cosimoangelo.greco@gmail.com
Article Info
Received: Jun 12, 2023
Accepted: Jul 06, 2023
Published: Jul 13, 2023
Archived: www.jclinmedsurgery.com
Copyright: © Angelo GC (2023).
Abstract...
Aorta–right atrial fistula is more commonly caused by endocarditis or aortic dissection and less commonly as a complication of aortic surgery. We report a rare case of aorta–right atrial fistula in a 54-year-old woman after a recent surgery of tricuspid valve repair. The tricuspid ring by its upper extremity close to the aortic root, produced an erosion of the aortic wall and the fistula. The surgeon must be aware of this possible serious condition to obtain the correct size and position of the prosthetic ring.
Keywords: Tricuspid valve; Prosthetic ring; fistula; Cardiac surgery; transesophageal echocardiography.
Abbreviations: TV: Tricuspid Valve; TR: Tricuspid Regurgitation; 3D: 3-Dimensional; TEE: Transesophageal Echocardiography; AR: Aortic Root; CS: Coronary Sinus; LA: Left Atrium; RA: Right
Atrium; IVC: Inferior Vena Cava; SVC: Superior Vena Cava.
Citation: Angelo GC, Aurora P, Federica M, Massimiliano G, Marco C, et al. Aorta-Right Atrial Fistula after Tricuspid Valve Repair. J Clin Med Surgery. 2023; 3(2): 1109.
Introduction
Aorta–right atrial fistula is a rare entity with anomalous connection between the aorta and the right atrium (RA) [1]. This anomaly may be congenital, more commonly secondary to conditions such as aortic dissection or infective endocarditis and less commonly as a complication of aortic surgery [1]. We report a case of aorto-right atrial fistula after tricuspid valve (TV) repair with prosthetic ring originating from non-coronary sinus of Valsalva.
Case report
A 54-year-old woman presented to our hospital for increasing dyspnea and lower limbs edema. Her past cardiac history included closure of interatrial septum defect in childhood and recent mitral and TV repair with two incomplete rings. In the last weeks, the patient had begun to develop fatigue and dyspnea with progressive difficulty to perform daily activity. Physical examination revealed a continuous murmur at the right upper sternal border. Transesophageal echocardiography (TEE) showed absence of residual mitral and tricuspid regurgitation (TR) and a systolic-diastolic flow between aorta and RA (Figure 1).
3-dimensional (3D) TEE reconstruction allowed to visualize a precise spatial position of fistula (between the non-coronary sinus of Valsalva and RA) and the adjacent structures. The fistula appeared close to the medial extremity of the Contour 3D tricuspid ring (Figure 2). We also found an inferior venous sinus type interatrial septal defect with left-to-right shunt, residual from surgical closure in childhood (Figure 3).
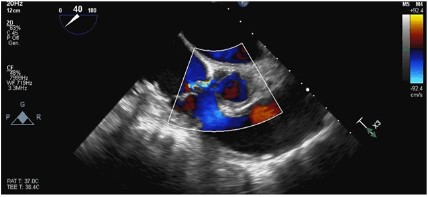
Figure 1: Systolic-diastolic flow between aorta and right atrium.
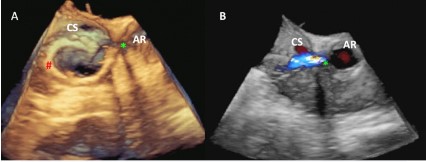
Figure 2: Aorta–right atrial fistula in 3-dimensional transesophageal echocardiography. AR: Aortic Root; CS: Coronary Sinus; red#: tricuspid ring; green*: fistula.
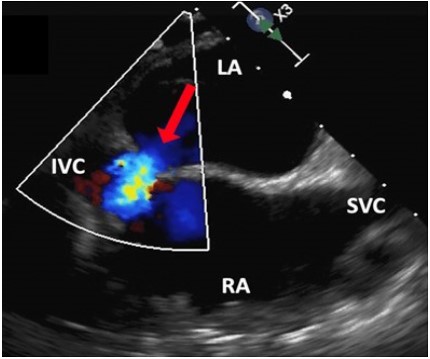
Figure 3: Inferior venous sinus type interatrial septal defect
with left-to-right shunt. IVC: Inferior Vena Cava; LA: Left Atrium;
RA: Right Atrium; SVC: Superior Vena Cava.
Considering the severity of patient's symptoms, cardiac surgery was performed to repair the fistula and the atrial septal defect. After sternotomy, the patient underwent extracorporeal circulation by cardiopulmonary bypass. The surgical inspection confirmed the 3D TEE anatomical reconstructions, and it demonstrated a supra-annular surgical suture of the tricuspid ring. No evidence of vegetations or abscess was found. The absence of any of the former was the reason for an iatrogenic cause was considered. The upper medial end of the tricuspid ring in contact with the Aortic Root (AR) procured an initial erosion and then the fistula. The fistulous road was demonstrated by a Klemmer clamp introduced from RA to AR (Figure 4) and it was closed by pledgeted suture. Given the absence of TR, the surgeon decided on not explanting the ring but simply cutting off its medial end. The interatrial defect was closed with direct suture.
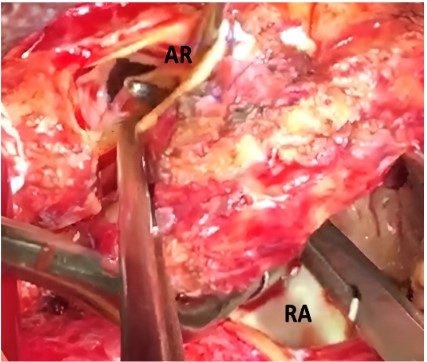
Figure 4: Surgical inspection of the fistula. AR: Aortic Root; RA:
Right Atrium.
Postoperative echocardiogram demonstrated preserved biventricular systolic function, correct position of the mitral and tricuspid rings with no regurgitation and absence of fistula flow. The interatrial septum was intact without a left-right shunt both in basal conditions and after infusion of agitated saline. The patient was extubated early and discharged in good hemodynamic compensation.
Discussion
Surgical TV repair is considered the gold standard for functional TR and tricuspid annuloplasty is the preferred technique [2]. More recently, 3D-shaped semi-rigid rings have been developed and used widely around the world [3]. Their more physiological 3D shape could combine the positive aspects of flexible and rigid rings, providing better results in terms of TR recurrence in the long term [3]. This prosthetic ring resembles the natural 3D shape of the TV annulus and it is designed to avoid interference with heart’s conduction system (Figure 5) [3]. The medial side of the ring is on a superior plane compared to the whole structure and near the AR. This shape may be at risk for this iatrogenic complication, because of possible aortic erosion if surgeon places the sutures in an upper position (too high in the anterior annulus), facing the ring’s medial extremity close to AR.
In literature, two other cases of aorta-right atrial fistula have been described as a consequence of TV repair but the number could increase in view of this growing interest in TV repair techniques [4,5]. Therefore, it seems essential to know this possible iatrogenic complication to prevent it.
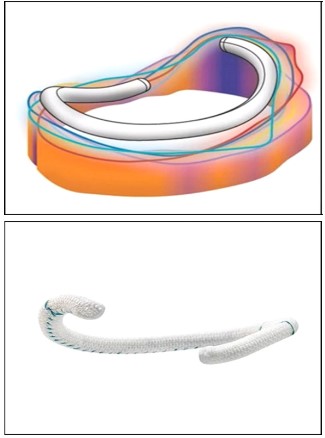
Figure 5: Contour 3D tricuspid ring.
Conclusion
Aorto-right atrial fistula is a rare complication after tricuspid prosthetic ring implantation but with important hemodynamic consequences for the patient. The surgeon must be aware of this possible serious condition to obtain the correct size and position of the prosthetic ring. The 3D TEE allows the diagnosis of fistula through a correct anatomical reconstruction and it directs the surgeon to successful repair.
Declarations
Conflict of Interest: Nothing to disclose.
Funding statement: Nothing to disclose.
Consent statement: The patient provided informed written consent for the publication.
References
- Fierro EA, Sikachi RR, Agrawal A, Verma I, Ojrzanowski M, Sahni S. Aorto-Atrial Fistulas: A Contemporary Review. Cardiol Rev. 2018; 26: 137-144.
- Arsalan M, Walther T, Smith RL, Grayburn PA. Tricuspid regurgitation diagnosis and treatment. Eur Heart J. 2017; 38(9): 634-638.
- Carino D, Zancanaro E, Lapenna E, Ruggeri S, Denti P, Iaci G, et al. Long-term results of tricuspid annuloplasty with 3-dimensional-shaped rings: Effective and durable! European Journal of Cardiothoracic Surgery. 2021; 60(1): 115-121.
- Menon PR, Doenst T, Ender J, Mohr FW, Mathioudakis D. Surgical Treatment of an Aorto-Right Atrial Fistula as a Complication of Tricuspid Valve Repair. Thorac Cardiov Surg. 2011; 59: 247-254.
- Wise J, van Helmond N, Awad AS, Peters PJ, Trivedi KC, Desai RD, et al. Aorto-right atrial fistula as a complication of tricuspid valve repair. J Cardiothorac Vasc Anesth. 2021; 35(2): 677-679