Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 3
Open Access
Volume 3
*Corresponding Author: GK Parvathidevi
Sri Siddhartha medical college & research center, Tumkur-572107, Karnataka, India.
Email: drgkparvathidevi27@gmail.com
Article Info
Received: May 22, 2023
Accepted: Jun 19, 2023
Published: Jun 26, 2023
Archived: www.jclinmedsurgery.com
Copyright: © Parvathidevi GK (2023).
Citation: Parvathidevi GK. Warthin-Like Papillary Thyroid Carcinoma: A Rare Case Report. J Clin Med Surgery. 2023; 3(1): 1105.
Introduction
Warthin-like papillary thyroid carcinoma, first described in 1995 by Aptel et al., is relatively uncommon variant of Papillary Thyroid Carcinoma (PTC) with about 81 cases reported in English literature to date [1-3]. The term “warthin tumor like PTC” was first coined on the basis of its close morphological resemble to warthin tumour, characterstically occuring in salivary glands. Cinically it usually presents as a cystic or solid cystic thyroid nodule. Histologically it is composed of papillae lined by large polygonal cells with abundant eosinophilic finely granular cytoplasm with a core exhibiting dense chronic inflamma- tory infiltrate, consisting of predominently of lymphocytes and plasma cells. Fine Needle Aspiration (FNAC) and the histological confirmation of warthin tumour like PTC can pose diagnostic difficulties in distinguishing these neoplasm, from a florid chronic thyroiditis. Hurthle cell nodules in chronic lymphocytic thyroiditis, hurthle cell tumours, tall cell and oncocytic variants of PTC and lastly oncocytic variant of medullary carcinoma. However the main diagnostic criterion for diagnosis of warthin - like PTC is the detection of the typical nuclear features commonly seen in conventional type PTC namely, optically clear nuclei, nuclear grooves and intra nuclear pseudoinclusions.
Case presentation
A- 45 -year old woman presented with Swelling on the anterior neck. Clinical evaluation revealed a diffuse thyroid mass involving whole of the gland. No lymph node enlargement was present. Thyroid function blood tests revealed a high level of thyroglobulin protein (280 ng/dl) with no abnormalities for FT3, FT4 and TSH. An ultrasound performed showed 5 x 4 x 3 solid cystic mass located in the left thyroid lobe.
FNAC showed cellular smears with follicular cells arranged in three dimensional groups, papillary fragments and single cells in the back ground of numerous reactive lymphocytes (Figures 1,2). These cells were polygonal to spindle shaped with abundant eosinophilic cytoplasm and large nuclei with finely dispersed chromatin and one or two prominent nucleoli, suggestive of oncocytic cells (Figures 3,4). Nuclear features of papillary carcinoma, that is nuclear chromatin clearing, membrane thickening, grooves and inclusions were evident in some of the cells (Figures 5,6). Some neoplastic cells were bi-or multi nucleated. Some amount of lymphocytes were present in the back ground (Figure 7). Cytological diagnosis was consistent with oncocytic variant of PTC. Patient underwent total thyroidectomy and was sent for histological examination.
Grossly both lobes of thyroid with isthmus were sent separately and were enlarged. The right lobe measured 5 x 3 x 2.5 cms. Left lobe with isthmus measured 5 x 2 x 1 cms (Figure 8). On cross section both lobes showed well circumscribed yellowish nodules measuring 4 cm and 3 cms in the greatest diameter respectively and covered by a thin rim of normal looking thyroid tissue.
Microscopically the tumour was well circumscribed and showed predominant papillary architecture. The tumour papillae were lined by oncocytic cells showing typical nuclear features of PTC, namely chromatin clearing, pseudonuclear inclusions and grooves (Figures 9,10). The papillary stalks were filled with dense inflammatory infiltrate, predominantly consisting of lymphocytes and plasma cells. The surrounding thyroid exhibited lymphocytic thyroiditis. Vascular invasion and invasion into the surrounding normal thyroid was not seen. Based on these features a diagnosis consistent with “warthin like- PTC “was rendered.
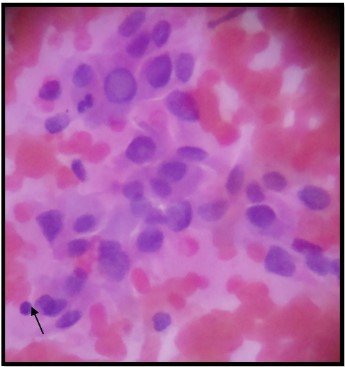
Figure 1: FNAC showing three dimentional papillary fronds
with lymphocytes (arrow) [H&E, 100X].
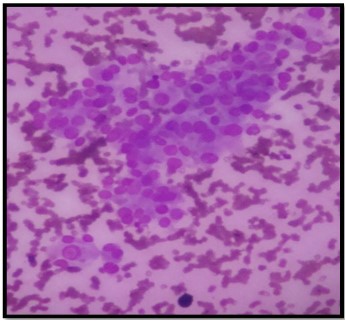
Figure 2: FNAC showing tumour cells [Leishman, 100x].
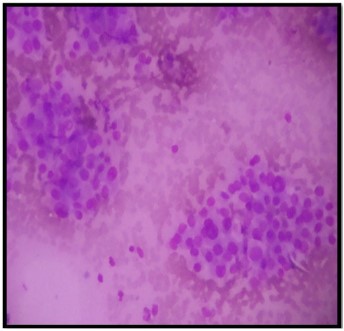
Figure 3: FNAC showing tumour cells and lymphocytes [Leishman, 100X].
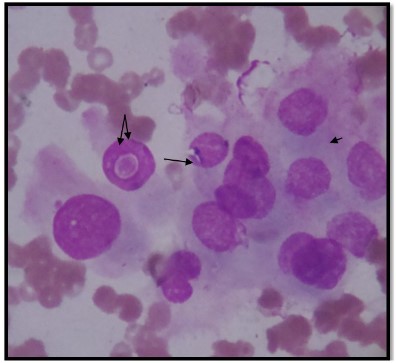
Figure 4: FNAC showing intranuclear inclusions (single arrow),
oncocytic cytoplasm, (double arrow) and grooves (small arrow)
[Leishman, 400x].
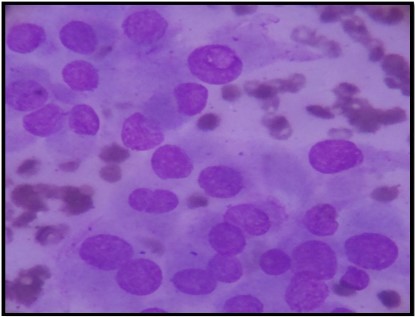
Figure 5: FNAC showing tumour cells and lymphocytes [Leishman, 400x].
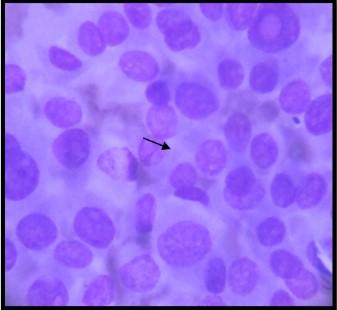
Figure 6a: FNAC showing tumour cells showing grooves (single
arrow) [Leishman, 400x].
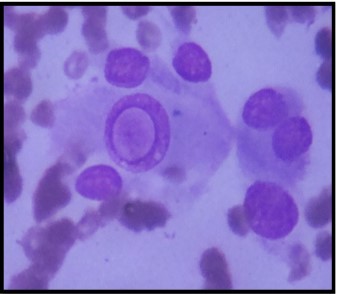
Figure 6b: FNAC showing intranucelar inclusions [Leishman,
400x].
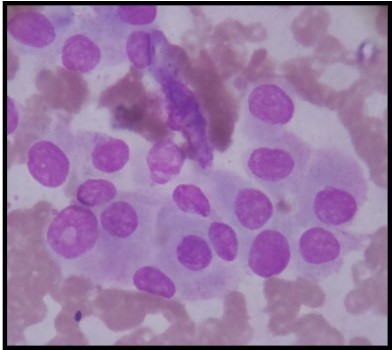
Figure 7: FNAC showing tumour cells with oncocytic cytoplasm.
[Leishman, 400x]

Figure 8a: Showing nodular yellowish mass.

Figure 8b: Showing cut section of tumour.
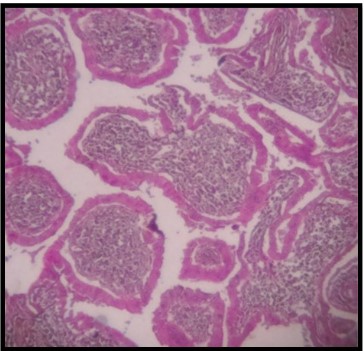
Figure 9: HPE showing papillae with lymphocytes and plasma
cells in the core [H&E, 100X].
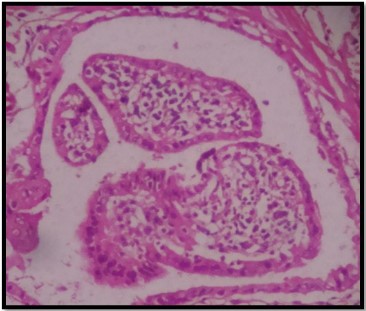
Figure 10a: HPE showing papillae lined by oncocytic cells and
core showing lymphocytes and plasma cells [H&E, 400x].
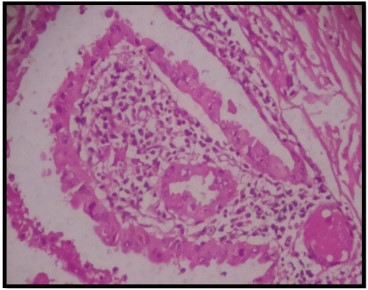
Figure 10b: HPE showing papillae lined by oncocytic cells and
core showing lymphocytes and plasma cells [H&E, 400x].
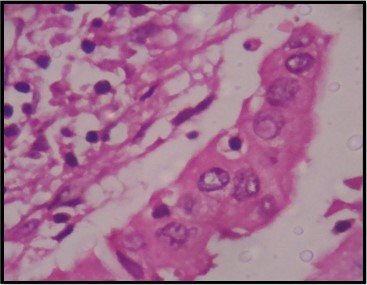
Figure 10c: HPE showing papillae lined by oncocytic cells and
core showing lymphocytes and plasma cells [H&E, 400x].
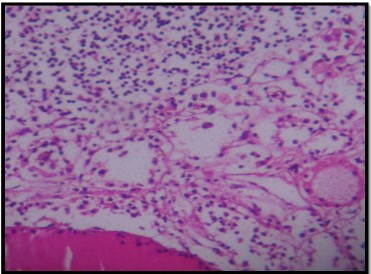
Figure 11: HPE of surrounding thyroid showing lymphocytic thyroiditis [H&E, 100X].
Discussion
Warthin tumour like PTC is a relatively uncommon variant of PTC [2]. These tumours are charecterised by papillary architecture, oncocytic tumour cells and nuclear features of papillary carcinoma. Carcinoma arising in the background of lymphocytic thyroiditis [3,4]. Apel et al coined the designation of this tumour in regard to its close resemblance to papillary cystadenoma lymphomatosum or Warthin tumour of salivary glands. The authors found that the epidemiological features of this variant of papillary carcinoma are similar to typical (classical) papillary carcinoma.
The tumour in our case was limited to thyroid, and had no evidence of vascular invasion or extra thyroidal extension and the followup period was one year which was uneventful. The available published data suggest that these tumours behave as usual papillary thyroid carcinoma with prolonged survival and excellent long term prognosis. The tumours with varying degrees of dedifferentiated components show aggressive biological behaviour an can lead to patient death [1]. Papillary carcinoma and its variants can exhibit different degrees of oncocytic metaplasia. Hurthle cell and tall cell variants of papillary carcinoma show prominent oncocytic change. Papillary hurthle cell carcinomas comprise one percent to eleven present of papillary carcinomas and are characterised by papillary architecture lined by oncocytic cells with nuclear features of papillary carcinoma.
However the usually lack the lympho-plasmacytic infiltrate and strong association with lymphocytic thyroiditis, as seen in warthin like variant [1-4]. The tall cell variant of papillary carcinoma is charecterised by papillary growth pattern, oncocytic enlarged tumour cells with height twice that of their width, papillary cancer nuclei. Clinically this variant of papillary cancer can behave in a more aggressive fashion and is frequently associated with extrathyroidal extension, vascular invasion, lymphnode and distant metastasis and tumour recurrence.
In both cytologic and histologic preparations, warthin like variant of papillary carcinoma can be mistaken for tall cell variant of papillary carcinoma owing to its oncocytic cytologic features [3,4]. The distinguishing features between these two entities include lack of elongated cells, presence of prominent nucleoli, granular cytoplasm and a concomitant lymphocytic infiltrate in the warthin like lesion [1].
Some hurthle cell lesions on the histologic sections can assume a pseudopapillary architecture due to collapse and disruption of their follicular architecture. These features are related to a paucity of tumour stroma in hurthle cell tumours (benign and malignant) as compared to other follicular cell derived tumours [1]. This pseudo papillary pattern can be mistaken for papillary hurthle cell carcinoma, which can alter the clinical management since the hurthle cell carcinomas behave in a more aggressive fashion than do papillary carcinoma. It is important not to over interpret papillary structures in hurthle cell neoplasms as papillary thyroid carcinoma. The appropriate nuclear features of papillary thyroid carcinoma must be present to diagnose a hurthle cell papillary cancer [1].
The presence of hurthle cells and lymphocytes can be seen in aspirates from lymphocytic thyrioditis. In addition, some of the cells may show nuclear enlargement and chromatin clearing due to reactive changes, which may lead to false positive diagnosis. However the tumours , especially papillary carcinoma arrising in the background of lymphocytic thyroiditis, usually show two cell population in cytology samples, namely tumour cells with nuclear features of papillary carcinoma and a background population of hurthle cells intermixed with small and large reactive lymphocytes [2].
Prominent cystic change can be seen in the main tumour mass. The combination of cystic lesion with a predominant lymphoid component arrising in the back ground of lymphocytic thyroiditis can be mistaken for a a benign lymphoepithelial cyst. These uncommon lesions are seen mainly in thyroids affected by lymphocytic thyroiditis. It has been suggested that they arrise from intra thyroidal branchial remnants. Lymphoepithelial cysts usually are lined by flattened squamous or respiratory epithelium and lack intracystic papillary growth pattern [1]. All these lesions are located in the lateral lobe of the gland, whereas warthin like papillary thyroid cancer can arrise in any area of the thyriod gland.
The presence of lymphocytic infiltrate within in the stalks of warthin-like papillary carcinoma imparts a distinctive appearence to this tumour [1-5]. Inflammatory infiltrates can be seen in association with other variants of papillary carcinoma. Some authors have suggested that this feature may be partly responsible for the indolent clinical course associated with papillary cancer. It has been showed that the malignant thyroid follicular cells express HLA type 11 antigens in response to tumour infiltrating lymphocytes, which may play a role in immune response against thyroid cancer. These studies although they represent a complex picture of tumour host interaction do suggest that tumour asssociated lymphocytes may play a role in the control of thyroid cancer; this role needs be defined later [1].
Conclusion
Warthin-like tumours can be mistaken for benign lymphoepihelial lesions of thyroid, hurthle cell carcinoma and tall cell variant of papillary thyriod carcinoma in both fine needle aspiration and histology specimens. Follow up information on the previously reported cases has suggested that these tumours behave similarly to usual papillary carcinoma. The extensive lymphocytic infiltration in these tumours and their association with chronic lymphocytic thyroiditis may suggest a role for immunological mechanisms in the pathogenesis of thyroid tumours.
References
- Baloch ZN, livoki VA. Warthin-like papillary carcinoma of thyroid. Arch Pathol and Lab Med. 2000; 124: 1192-1195.
- Amico P, Lanza fame S, Destri GL, Greco P, Caltabiano R, et al. Warthin like papillary thyroid carcinoma with a minor dedifferentiated component: Report of a case with clinic pathological considerations. Hindawi Publishing Corporation. Case reports in medicine. 2010; 495281: 5.
- Fadda G, Mule A, Zannoni GF, Vincenzoni C, Ardito G, etal. Fine needle aspiration of warthin like thyroid tumour: report of a case with differential diagnostic criteria vs other lymphocytic rich thyriod lesions. Actacytol. 1998; 42: 998.
- Vera- sempere FJ, Prieto M, Camanas A. Warthin like tumour of thyroid, a papillary carcinoma with mitochondrial rich cells and abundant lymphoid stroma: A case report. Pathol Res Pract. 1998; 194: 341.
- Vasei M, kumar PV, Malekhoseini SA, Kadivar M. Papillary hurthle cell carcinoma (warthin-like tumour) of the thyroid. Acta cytol. 1998; 42: 1437.