Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 3
Open Access
Volume 3
*Corresponding Author: GK Parvathidevi
Sri Siddhartha medical college & research center, Tumkur-572107, Karnataka, India.
Email: drgkparvathidevi27@gmail.com
Article Info
Received: May 22, 2023
Accepted: Jun 15, 2023
Published: Jun 22, 2023
Archived: www.jclinmedsurgery.com
Copyright: © Parvathidevi GK (2023).
Citation: Parvathidevi GK. Cytodiagnosis of Primary Hodgkin’s Lypmhoma arising in Warthin’s Tumour. J Clin Med Surgery. 2023; 3(1): 1104.
Introduction
Warthin’s tumour is a benign neoplasm with a proliferative epithelial component of salivary gland epithelium and lymphoid stroma [1]. It is commonly found in the lower pole of the parotid gland, and an estimated 12-20% are multicentric and 5-14% are bilateral [2-4].
Approximately, 1% of warthin’s tumour undergo malignant transformation which can be seen in both the epithelial and lymphoid components [5]. Some studies indicate a higher frequency of malignant transformation in the lymphoid components, others indicate that non-Hodgkin’s lymphoma diagnosed in WT excision material is almost rare [1-4]. Only one case of Hodgkin’s disease occurring in a WT is reported in literature [6].
Furthermore, literature shows one case of WT with co-existent Hodgkin’s disease [7].
Here we describe a case of Hodgkin’s lymphoma arising in WT in a 50-year-old male patient. Which forms 2nd such case report in English literature.
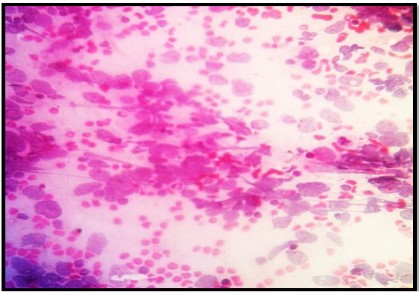
Figure 1: FNAC showing pleomorphiclymphoid cells (H&E, 40X).
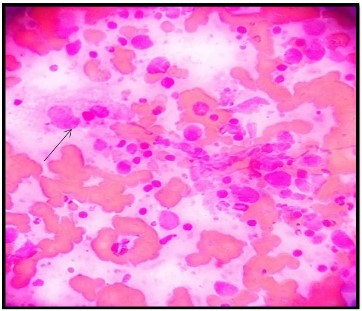
Figure 2: FNAC showing polymorphous population of cells with
RS cell (arrow) (Leishman, 40X).
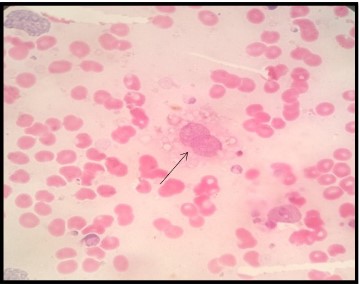
Figure 3: FNAC showing RS cells (arrow) (H&E, 40X).

Figure 4: Showing lobulated tumour mass.

Figure 5: Cut section showing gray-white areas with tiny cystic
spaces (arrow).
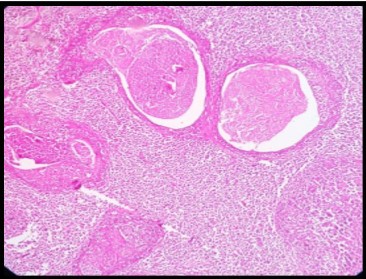
Figure 6: HPE showing multiple cystic spaces lined by oncocytic
epithelium (arrow) (H&E,10X)
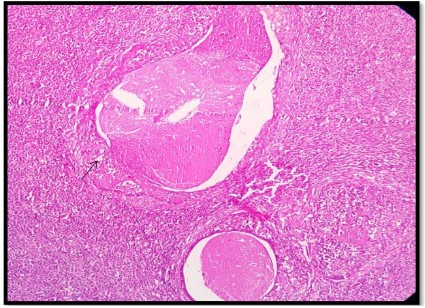
Figure 7: HPE showing cystic spaces lined by oncocytic epithelium (arrow) (H&E, 10X).
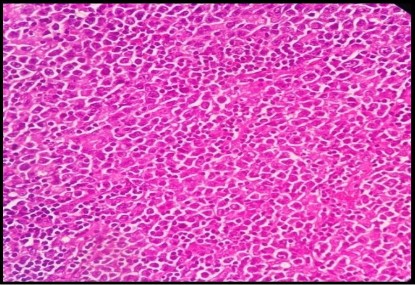
Figure 8: HPE showing pleomorphic lymphoid cells (H&E, 40X).
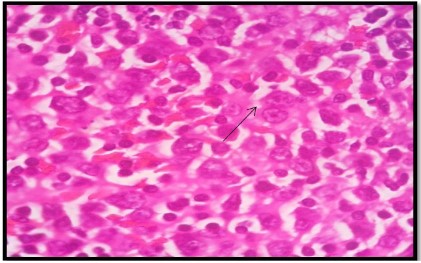
Figure 9: HPE showing RS cells (arrow) (H&E, 100X)
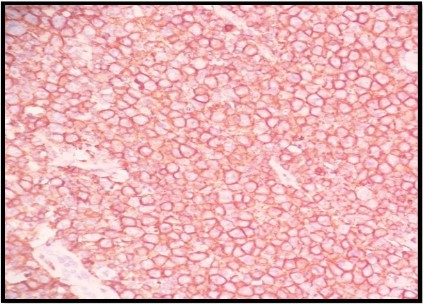
Figure 10: IHC showing CD20 positivity.
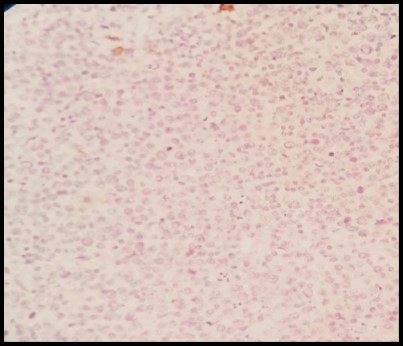
Figure 11: IHC showing EMA negativity.
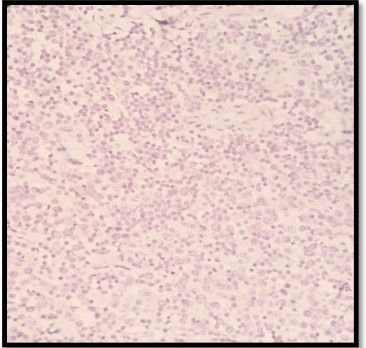
Figure 12: IHC showing CK20 negativity.
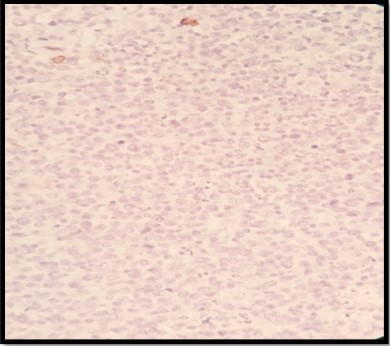
Figure 13: IHC showing CD3 negativity.
Case presentation
A 50-year-old male patient presented with a painless swelling in the left parotid region for the last 1 year. On examination a mass of 5 x 5 cms was identified in the left parotid region. It was non tender fixed and soft to firm to hard in consistency. There were no lymph nodes enlarged and there was no evidence of sjogren’s syndrome.
Hematological investigations were within normal limits (Hb12.2 gm/dl, total leucocyte count-4900 cumm & a differential count of 70% neutrophils, 25% lymphocytes, 03% eosinophils & 02% monocytes, platelet count 1.7 lakhs/cumm). His ESR was elevated with 55 mm at the end of first hour. Computed tomography (CT) revealed a lobulated cystic mass of 8 x 6 x 3 cm arising from the deep lobe of the parotid.
FNAC smears were moderately to highly cellular and comprised of polymorphous populationof large atypical lymphoid cells with high NC ratio, irregular nuclear contour, vesicular chromatin, prominent nucleoli & scant cytoplasm admixed with scattered neutrophils, eosinophils & plasma cells (Figures 1,2). At places, binucleate Reed Sternberg cells were seen (Figure 3), along with few clumps of oncocytic epithelial cells. A diagnosis of Hodgkin’s Lymphoma was offered. Subsequently, parotid mass was excised.
Grossly it was lobulated ovoid mass measuring 7 x 6 x 4 cms (Figure 4). Cut section was grey white with tiny cystic spaces (Figure 5).
Microscopy showed tumour tissue interspersed with cystic spaces, which are lined by oncocytic epithelium (Figures 6,7). Tumour tissue was composed of polymorphous population of pleomorphic lymphoid cells admixed with neutrophils, eosinophils& plasma cells. At places Reed-stern berg cells were seen (Figures 8,9). Some of the cystic spaces filled with pink granularproteinaceous material and cholesterol clefts. A diagnosis of Hodgkin’s lymphoma arising from Warthin’stumours was made.
Subsequently bone marrow biopsy was done and it was found to be free of tumour.
Co-relating clinical history, radiological finding, final diagnosis of Hodgkin’s lymphoma arising in warthin’stumour of left parotid gland was made.
Subsequently, immunohistochemistry was performed. The neoplastic cells expressed CD20 (Figure 10) and were negative for CD3, EMA and CK20 (Figures 11,12,13). The patient was referred to higher centre for chemotherapy, he was treated with 6cycles of chemotherapy & is on maintenance therapy and is doing well.
Discussion
Carcinoma arising in a pleomorphic adenoma is well known but malignant transformation in WT is rare [8]. The incidence of WT is 11.5% of all parotid tumours and the incidence of malignant transformation WT was 1.1% in one series [9]. Malignant transformation is rarer in lymphoid component than the epithelial component. Malignant lymphoma apparently arising in lymphoid component is extremely rare. Some cases have no remnant of the lymphoid component, which normally occurs in WT, as this was totally replaced by malignant lymphoma in the advanced disease [4]. In our case also lymphoid stroma was totally replaced by malignant lymphoma and the epithelial component was recognizable as cyst lining oncocytic epithelium.
The pathogenesis of malignant transformation of WT remains unclear. However exposure to radiation is of particular interest, as the relationship between previous radiotherapy and lymphomas arising from WT has been determined by some authors [1]. Chronic immune sialadenitis is thought to play an important role, independent of the presence of sjogren’s syndrome symptoms [4]. In our case, there was no history of radiotherapy or sialadenitis or smoking.
Saxena et al., stated that because the lymphoid stroma of WT is part of systemic lymphoid tissue, in patients with lymhomatous spread of WT, disseminated disease is present during the staging either at the time of diagnosis or later [1].
In our case bone marrow biopsy showed no disease involvement. Screening doesn’t reveal any lymphadenopathy in any other site, indicating no disseminated disease, present synchronously.
It has been suggested that lymphomas seen with WT are typically non-hodgkin’s lymphomas; however there are a few cases reporting Hodgkin’s lymphoma [6,7]. Ours is 2nd case report in literature.
Conclusion
Malignant lymphomas in WT are very rare. The presented case is Hodgkin’s lymphoma expressing CD20 positivity. To the best of our knowledge, this is the second case in literature describing Hodgkin’s lymphoma with expression of CD20 in WT.
References
- Ozkok G, Tash F, Ozsan N, Ozturk R, Postaci H. Diffuse large B-cell lymphoma arising inwarthin’stumours: Case study & review of literature. The Korean Journal of pathology 2013; 47: 579-582.
- Rosai J. Major and minor salivary gland. In: Rosai J, ed. Rosai and Ackerman’s Surgical pathology 10th ed. Edinburg: Elsevier. 2011; 826-828.
- Cheuk W, Chan JK. Salivary gland tumours. In: Fletcher CD, ed. Diagnostic histopathology of tumours 3rd ed. Philadelphia: Churchill livingstone Elsevier. 2007: 266-269.
- Gorai S, Numata T, Kawada S, Nakano M, Tamaru J, et al. Malignant lymphoma arising from heterotrophic warthin stumours in the neck: Case report and review of literature. Tohoku J Exp. Med. 2007; 212: 199-205.
- Simpson RH, Eveson JW. Warthintumour. In: Barnes L, Eveson JW, Reichart P, Sidransky D, eds. Pathology and genetics head and neck tumours: World Health Organisation classification of tumours. Lyon Press. 2005; 263-2655.
- Melato M, Falconieri G, Fanin R, Baccarani M. Hodgkin’s disease occurring in a Warthin’stumour: First case report. Pathol Res Pract. 1986; 181: 615-620.
- Badve S, Evans G, Mady S, Copper M, Sloane J. A case of Warthin’stumour with coexistent Hodgkin’s disease. Histopathology. 1993; 22: 280-281.
- Nagao K, Matsuzaki O, Saiga H, Sugano I, Shigematsu H, et al. Histopathologic studies on carcinoma in pleomorphic adenoma of the parotid gland. Cancer. 1981; 48: 113-121.
- Nagao T, Sugano I, Ishida Y, Tajima Y, Furuya N, et al. Mucoepidermoid carcinoma arising in Warthin’s tumour of the parotid gland: report of two cases with histopathological, ultrastructural and immunohistochemical studies. Histopathology. 1998; 33: 379-386