Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 3
Open Access
Volume 3
Dianda D; Guelfi R; Corti F; Gatta L; Perotti B*; Arganini M
*Corresponding Author: Perotti B
Gastroenterology of Versilia Hospital, AUSL Toscana Nord-Ovest, Lido di Camaiore (LU), Italy.
Email: bruno.perotti@uslnordovest.toscana.it
Article Info
Received: Apr 14, 2023
Accepted: May 08, 2023
Published: May 15, 2023
Archived: www.jclinmedsurgery.com
Copyright: © Perotti B (2023).
Citation: Dianda D, Guelfi R, Corti F, Gatta L, Perotti B, et al. Laparoscopic Surgical Treatment of Hiatal Hernia with Gastric Volvulus: Report of a Case. J Clin Med Surgery. 2023; 3(1): 1094.
Introduction
Paraesophageal hernias represent 5 to 10% of all hiatal hernias. Mainly because of the ageing of the population, their incidence is increasing: the etiopathogenesis is defined in fact by weakening of the diaphragmatic esophageal ligament, dilatation of the esophageal hiatus due to vertebral body fracture, gibbus deformity, obesity, and an increase in abdominal pressure [2]. They are classified into four types [1]:
- Type I, sliding hiatal hernias, is the most common (approximately 95% of the cases). There is a circumferential laxity of the phrenoesophageal membrane and widening of the muscular hiatal tunnel, allowing a portion of the gastric cardia to herniate upwards;
- Type II, pure paraesophageal hiatal hernia, the gastric fundus herniates into the thorax. The gastroesophageal junction maintains its natural position;
- Type III, mixed hiatal hernia, which are most common in older women, is the association of type II with the migration of the gastroesophageal junction into the thorax;
- Type IV, complex hiatal hernia, is characterized by the migration of other viscera through the hiatus which is defined Giant hiatal hernia: a condition in which one-third or more of the stomach migrates into the thorax [2]. Other intra-abdominal organs, such as colon, spleen and small intestine, can be involved in the herniation Primary giant hiatal hernia can lead to chronic low-grade symptoms such as, abdominal pain, passage disorder, anemia, strangulation, and aspiration pneumonia, early satiety, heartburn, dysphagia, dyspnoea, chest discomfort or can be asymptomatic.
The pathophysiology of hiatal hernia is still unclear: congenital or acquired widening of the diaphragmatic hiatus (weakness of the muscular crura due to elastin, collagens and matrix metalloproteinases abnormalities) and the increasing of intra-abdominal pressure are the most frequent causes. In the elderly, indeed, paraesophageal hernia is often asymptomatic, and the debate on whether to treat or not an asymptomatic patient is still active, following the high mortality and morbidity rate in elective repair. The symptoms, associated with the inability to progress the nasogastric tube, make up Borchdat’s triad, consisting in retching, epigastric pain and failure to place a nasogastric tube, present in 70% of cases. If the symptoms are present, there is a very indication for elective surgical treatment. Severe acute symptoms are very uncommon [3,4]. Hematemesis can occur as a result of mucosal ischemia associated with vomiting. Complications include ulceration, perforation, pancreatic necrosis and omentum avulsion Among the cases of esophageal hiatal hernia, relatively few cause respiratory and circulatory disorder [5]. Nevertheless, cases requiring emergency surgery include those where patients exhibit an incarcerated hernia, a prolapse, a gastric axis twist, a respiratory disorder due to lung compression and arrhythmia due to cardiac compression [6]
According to The Society for Gastroesophageal Reflux Disease in Japan conducted a national survey which declamed that hiatal hernias occur in 49.3% of individuals who undergo upper endoscopies. Therefore, careful consideration is required when deciding the course of treatment for esophageal hiatal hernias in older adults [7].
Literature suggests that patients with acute paraesophageal hernia have often average body mass index from 29 to 30 kg/m2 and with an American Society of Anaesthesiologists (ASA) score of III or higher (69–100%) [1].
Discussion
In particular, regarding the anatomical classification, the gastric volvulus can be organoaxial or mesenteroaxial, according to the rotation of the organ. In 60% of cases, rotation is characterized by rotation about the longitudinal axis, with the fixation points being the esophagogastric junction and the pylorus. And this is organoaxial rotation. In 30% of cases, rotation occurs mesenteroaxial, characterized by rotation about the transverse axis, pylorus under the esophagogastric junction and overlapping antrum. In 12% of cases, the two types of rotation coexist.
Rarely, giant hiatal hernia may present as an acute emergency due to the intrathoracic twisting of the stomach followed by mechanic obstruction. Haemorrhage (mucosal bleeding of the stomach), gastric ischemia and perforation, are severe sequelae of strangulation or upside-down stomach [5,6]. All these complications represent real life-threatening conditions, with a high mortality rate (up to 30%) [8].A chest-abdominal contrast-enhanced CT scan (Figure 4), and upper endoscopy are the most important exams to be performed during the pre-operative workup. Anyway, chest X-ray should be the first diagnostic tool to rule out other diagnoses and to detect perforating signs [1].
Endoscopy, trying a conservative management, having a direct view of mucosal condition (gastric ischemia). The clinical evolution is represented by bleeding or gastric perforation, with septic sequelae, if treatment is delayed. According to the selected articles, respiratory failure or even sepsis and shock are other possible acute presentations that appear to be the evolution of gastric ischemia: these unstable patients are often obliged to undergo open emergency surgery.
Gastric volvulus is a rare condition defined as an abnormal stomach rotation around its axis, which usually presents in adults in their fifth decade in children or under a year. Cases over 70-year-old are rare and only 30% of cases of this disease present with mesenteric-axial rotation of the stomach. Because of the risk of strangulation, the outcome can present as perforation and hypovolemic shock or necrosis with a mortality rate reaching 30 to 50%, requiring early diagnosis and approach [10]. Totally intrathoracic stomach hernias generally present such a risk of volvulus, strangulation, and perforation that surgery is indicated even in asymptomatic and uncomplicated cases. Although the pathophysiology is different, the Nissen procedure is the surgical procedure of choice for both types of hiatal hernia.
Laparoscopic approach to symptomatic patients with hiatal hernia gives its low mortality and morbidity and has gained broad consent. Laparoscopy is now considered the gold standard for elective surgery, since its first description in 1992 [1]; especially in clinically stable patients, it is considered safe also in an emergency setting [2]. However, in the case of unfit or unstable patients, the open approach remains mandatory. Even the robot-assisted approach, when available, giving the post-operative benefits of minimally invasive procedures (Figure 5], may represent a very valid option [9]. In a recent multi-institutional database study from the USA, robotic-assisted repair accounted for the 6% of all emergent cases and 8% of all minimally invasive treated ones [2]. Nevertheless, no previous article, among the selected ones, ever reported a predominant robotic approach for the emergent paraesophageal hernia repair. Age was not an exclusion criterion to minimally invasive approach. In the acute setting, the concerns about the postoperative risk of recurrence are negligible compared to the risk of gastric perforation (after gastric vascular sufferance) and the absence of functional study (oesophageal manometry, swallow x-ray exam, etc.). Factors such as presence of a high obstruction syndrome of the gastrointestinal tract and the chronicity of the condition, in addition to the patient’s age and high surgical risk, were decisive for choosing this surgical technique. Thus, a smaller surgical procedure was prioritized, aiming at a lower rate of possible postoperative complications.
General surgical treatment
The hiatal defect closure (direct or with mesh) may be followed by an anti-reflux procedure (according to Toupet or Nissen or Belsey-MK IV) or gastropexy. Surgical emergency treatment provides the reduction of the migrated stomach with the excision of the hernia sac [11]. Since the introduction of prosthetic mesh reinforcement is overall accepted that reduced the risk of recurrences [12]. Collis-Nissen procedure may be necessary due to the presence of oesophageal shortening [13]. Necrotic gastric wall or perforation may require gastric resection so that a fundoplication should be avoided. About fundoplication, the main factors that influence the decision are gastric fundus tissue condition and the history of GERD. Nissen fundoplication is reported up to 75–100% of cases and is the most common technique. Another approch is antireflux gastroplasty according to Dor: the gastric fundus is first anchored with three points to the left edge of the myotonia, then it is overturned on the anterior wall of the esophagus and is stabilized in this position with three points, symmetrical to the previous ones, which fix it to the right edge of the myotomy. Also in this phase, caution must be exercised in avoiding the entrapment of the vagus nerve in the most cranial points.
Additional techniques, such as gastrostomy, gastropexy, Collis procedure or gastric resections, are required in selected cases, and this underlines to what extent this surgery is tailored case by case.
Recently, pre-treatment patients’ characteristics were used to create a mortality and significant morbidity predictive model for giant hiatal hernia repair: the 2013 Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) guidelines recommend repair of all symptomatic paraesophageal hernias [13].
Emergency surgery for incarcerated-strangulated giant hiatal hernia is mandatory especially in the presence of the classic Borchardt’s triad. Generally, the patients present acutely with thoracic/abdominal pain and symptoms upper gastrointestinal bleeding (17–25%) [14] of mechanical gastric outlet obstruction (20–100%) [15].
There are no clear recommendations on the operative management of incarcerated hiatal hernia. Management algorithms for acutely presenting paraesophageal hernia were proposed on the results of a small series of patients. The increased perioperative mortality and morbidity associated with the emergency repair for gastric volvulus and strangulation are reported in many series [16]. Immediate open surgery is suggested in case of unstable patients. In other cases, emergent laparoscopic hiatal hernia reduction and repair may be carried out in cases without gastric perforation, with low morbidity rate and with the benefits of a minimally invasive approach [17]. The selected literature reported an average hospital stay of 4-9 days, overall morbidity rate of 0–52% and a recurrence rate of 0–17% [1].
With a few exceptions [18], a hiatoplasty is always performed with different suture strategies (direct, pledgets and meshes). There is no evidence regarding the advisable use and type of mesh: both synthetic and biologic mesh [19] have been adopted.
The surgical goals, indeed, appear to be different case by case, and techniques should be carefully tailored.
The choice of the best surgical technique for the treatment of gastric volvulus depends on each case, mainly taking into account factors such as the chronicity of the volvulus and its etiology.
Case report
Here we report a case of a 73-year-old female patient who was being evaluated for caffean vomit, abdominal pain and pancreatic cleavage. An abdominal RX confirmed gastrectasia and hydro-air levels of the colon. The patient was also subjected to abdominal CT which reported:
“Gross paraesophageal jatal hernia with cardia in place. The hernia goes up to the subcarinal site. The nasogastric tube stops at the cardia. Presence of gastrectasia with double organ-axial anthro-pyloric gastric volvulus with consequent stretched appearance of the duodenum” (Figure 1,2).
After endoscopic examination that could not proceed after gastric fundus due to adherences, a Laparoscopic exploration was performed. A Permagna paraesophageal hiatal hernia with intrathoracic gastric volvulus was identified (Figure 3), and we proceed to reduction in the abdomen of the stomach with devolvolation (Figure 4), no persistent signs of ischemia were detected; the hernial sac is isolated and removed after dissecting the diaphragmatic pillars, until the esophagus is passed through with a tape; posterior hiatoplasty of the large hiatal port (Figure 5) with two points in non-resorbable material and floppy fundoplication according to Nissen was performed.
Conclusion: The operative time was 130 minutes, and there was not significant blood loss. Postoperatively, the patient recovered well and was discharged by the eight postoperative day. To date the patient is in good health and disease free; control RX transit six days after surgery reported that the passage of water-soluble contrast agent (gastrografin) administered orally through the esophagus was regulated, not spreading opacification of the gastric lumen and of the first intestinal loops.
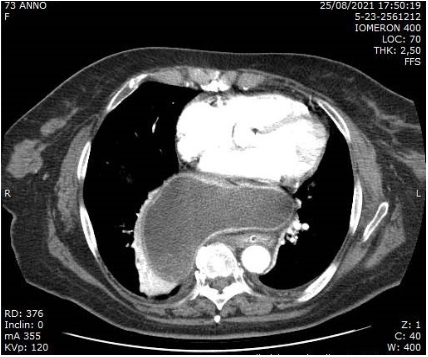
Figure 1: Gross paraesophageal jatal hernia with cardia in place.
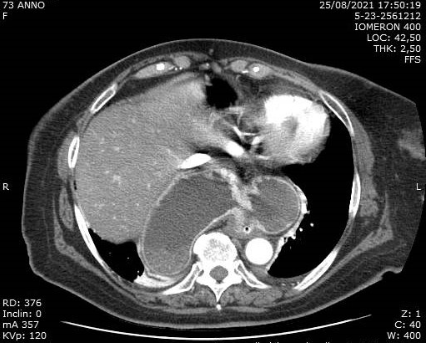
Figure 2: Double organ-axial anthro-pyloric gastric volvulus with
consequent stretched appearance of the duodenum.
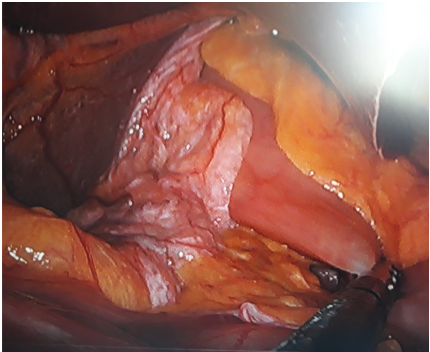
Figure 3: Permagna paraesophageal hiatal hernia with intrathoracic gastric volvulus.
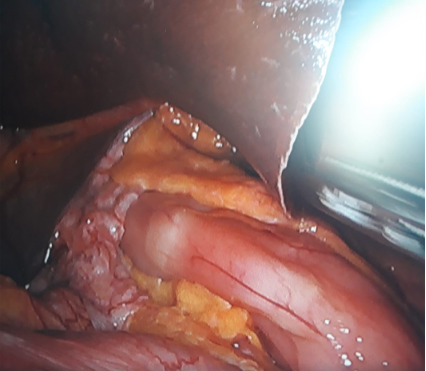
Figure 4: Reduction in the abdomen of the stomach with devolvolation.
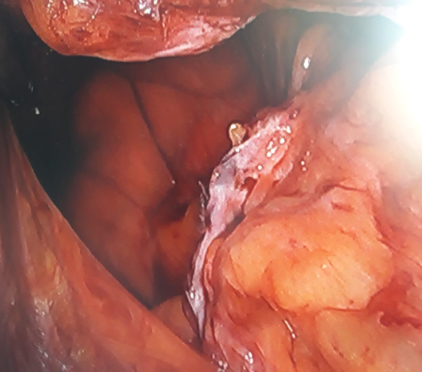
Figure 5: laparoscopic view of the hernial port.
Conclusions
Limited number of cases prevents from drawing any general conclusion. The robotic-assisted approach in acute paraesophageal hernia repair may give advantages compared to conventional laparoscopy, for what concerns the surgeon’s comfort and precision, and this is probably unique in emergency surgery. However, its use mainly depends on device availability and the surgical team’s experience. Moreover, no open procedures were accounted both in emergency and in elective setting, so any comparison was not possible. Still, the selected literature shows the absence of comprehensive data about the outcome after emergent robotic-assisted repair of giant hiatal hernia.
On the basis of current literature, in many cases, a minimally invasive approach is possible and safe, with good peri- and post-operative outcomes [1].
The laparoscopic approach is appropriated even in emergency and comprises complete reduction of the stomach in abdomen, making of effective hiatus-pasty, control of suitable position of the distal esophagus and cardias [2].
References
- Ceccarelli G, Pasculli A, Bugiantella W, De Rosa M, Catena F, et al. Minimally invasive laparoscopic and robot-assisted emergency treatment of strangulated giant hiatal hernias: report of five cases and literature review. World J Emerg Surg. 2020; 15: 37.
- Arcieri S, Palazzini G, Romani AM, Orsi E, Belfiore C, et al. Trattamento chirurgico minivasivo d’urgenza di ernia gastrica iatale paraesofagea strozzata. Caso clinico [Mininvasive treatment of strangulated paraesophageal hiatal hernia in emergency. Case report. G Chir. 2005; 26: 438-442.
- Luketich JD, Nason KS, Christie NA, Pennathur A, Jobe BA, et al. Outcomes after a decade of laparoscopic giant paraesophageal hernia repair. J Thorac Cardiovasc Surg. 2010; 139: 395-404.
- Larusson HJ, Zingg U, Hahnloser D, Delport K, Seifert B, et al. Predictive factors for morbidity and mortality in patients undergoing laparoscopic paraesophageal hernia repair: age, ASA score and operation type influence morbidity. World J Surg. 2009; 33: 980-985.
- Shafii AE, Agle SC, Zervos EE. Perforated gastric corpus in a strangulated paraesophageal hernia: a case report. J Med Case Rep. 2009; 3: 6507.
- Díez Ares JÁ, Peris Tomás N, Estellés Vidagany N, Periáñez GD. Gastric necrosis secondary to strangulated giant paraesophic hiatal hernia. Rev Esp Enferm Dig. 2016; 108: 498-500.
- Horinishi Y, Shimizu K, Sano C, Ohta R. Surgical Interventions in Cases of Esophageal Hiatal Hernias among Older Japanese Adults: A Systematic Review. Medicina (Kaunas). 2022; 58: 279.
- Sheff SR, Kothari SN. Repair of the giant hiatal hernia. J Longterm Effects Med Implants. 2010; 20: 139-148.
- Hosein S, Carlson T, Flores L, Rodrigues Armijo P, et al. Minimally invasive approach to hiatal hernia repair is superior to open, even in the emergent setting: a large national database analysis. Surg Endosc. 2020.
- Mori T, Atomi Y. Laparoscopic repair of esophageal hiatal hernia. Nihon Geka Gakkai Zasshi. 2003; 104: 587-92.
- Banki F. Giant paraesophageal hiatal hernia: a complex clinical entity. J Thorac Cardiovasc Surg. 2017; 154: 752-753.
- Gimenez FY, Takahashi LAR, Oliveira GG, Myaki JY, Inaba ME, et al. Hiatus hernia with gastric volvulus and duodenum component: a case report. J Surg Case Rep. 2021; 2021: rjab548.
- Kohn GP, Price RR, DeMeester SR, Zehetner J, Muensterer OJ, et al. SAGES guidelines committee. Guidelines for the management of hiatal hernia. Surg Endosc. 2013; 27: 4409-4428.
- Arevalo G, Wilkerson J, Saxe J. Acute paraesophageal hernia: laparoscopic repair with adjunct T-fastener gastropexy for the high operative risk patient. Surg Laparosc Endosc Percutan Tech. 2018; 28: 123-127.
- Shea B, Boyan W, Decker J, Almagno V, Binenbaum S, et al. Emergent repair of paraesophageal hernias and the argument for elective repair. JSLS. 2019; 23.
- Poulose BK, Gosen C, Marks JM, Khaitan L, Rosen MJ, et al. Inpatient mortality analysis of paraesophageal hernia repair in octogenarians. J Gastrointest Surg. 2008; 12: 1888-1892.
- Klinginsmith M, Jolley J, Lomelin D, Krause C, Heiden J, et al. Paraesophageal hernia repair in the emergency setting: is laparoscopy with the addition of a fundoplication the new gold standard? Surg Endosc. 2016; 30: 1790-1795.
- Light D, Links D, Griffin M. The threatened stomach: management of the acute gastric volvulus. Surg Endosc. 2016; 30: 1847-1852.
- Horstmann R, Klotz A, Classen C, Palmes D. Feasibility of surgical technique and evaluation of postoperative quality of life after laparoscopic treatment of intrathoracic stomach. Langenbeck’s Arch Surg. 2004; 389: 23-31.