Journal of
Clinical & Medical Surgery
Clinical & Medical Surgery
www.jclinmedsurgery.com
ISSN 2833-5465
Open Access
Volume 3
Open Access
Volume 3
*Corresponding Author: Amélie MEUNIER
Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital Center, 2 avenue Martin-Lu-ther-King, 87000 Limoges, France.
Email: chymaoby@yahoo.com
Article Info
Received: Dec 23, 2022
Accepted: Jan 20, 2023
Published: Jan 30, 2023
Archived: www.jclinmedsurgery.com
Copyright: © Meunier A (2023).
Abstract...
Introduction: Age-related processes in the oral mucosa increase the risk of cancer. The gingiva is the most common localization in the upper aerodigestive tract in the elderly. The aim of this study was to compare the patient and the tumor characteristics, treatments, disease-free survival, and overall survival for gingival squamous cell carcinoma in patients less than and older than 70 years of age.
Methods: This retrospective, observational, bicentric study included gingival squamous cell carcinoma cases diagnosed between 2007 and 2017. The population was divided into two age groups for the analysis.
Results: The elderly group included more women, non-smokers, and non-drinkers (p < 0.001). The histopathological characteristics were the same in both age groups, as was the T classification (p = 0.89). The younger group had more advanced nodal involvement (p = 0.01). After surgical treatment, the older patients received less adjuvant treatment (p = 0.001). Disease-free survival was better for the younger patients (p = 0.02) but there was no difference in overall survival. Deaths due to the treatment were more frequent in the elderly group (p = 0.007).
Conclusion: Gingival carcinomas in the elderly have specific features. Local control of the disease must be balanced with the increased toxicity of treatments.
Keywords: Elderly; Gingiva; Head and neck squamous cell carcinoma; Tobacco; Aging.
Abbreviations: DFS: Disease-Free Survival; EG: Elderly Group; OS: Overall Survival; SCC: Squamous Cell Carcinoma; YG: Younger Group.
Citation: Meunier A. Does Gingival Carcinoma in the Elderly Correspond to a Distinct Entity? J Clin Med Surgery. 2023; 3(1):1070.
Introduction
Head and neck cancers in elderly patients are a challenge, especially due to the increased frequency of cancer in this population. Gingival SCC is the most common localization of the upper aerodigestive tractin patients aged 70 and older [1].
The frailty and the comorbidities of these patients need to be considered in the therapeutic choice. Indeed, the current treatments can exert considerable toxicity, and there is a risk of undertreatment of this population [2].
The mucosa of the oral cavity is subject to age-related processes such as cellular aging and immunosenescence [3-6]. For some authors, increasing age, particularly above 60 years, should be considered to be a risk factor for the development of oral squamous cell carcinoma [3,7], although the exact role of aging in the carcinogenic process remains unknown. Gingival and cheek mucosa localizations are more frequent in the elderly [8]. Many hypotheses have been put forward, such as an increased mutational load, exposure to carcinogens, diminished awareness, inadequate nutrition, and altered immunity [3].
Oral SCC, and particularly a gingival mandibular mucosa localization, appear to be a common feature in the elderly, with a different natural history, whereby more women are affected, there has been no direct exposure to tobacco [9], and in our clinical impression they have multiple recurrences but no study is available about this last element. The identification of a particular population could lead to personalized treatments being developed that are tailored to elderly patients instead of a default reliance on major surgery, which is presently the standard treatment for oral cavity squamous cell carcinoma.
The aim of this study was to compare the patient and the tumor characteristics, the treatments received, the disease-free survival, and the overall survival for gingival SCC in patients less than and older than 70 years of age.
Material and methods
Three hundred and sixty patients with gingival SCC, diagnosed between the 1st of January 2007 and the 31st of December 2017, were included in this observational, descriptive, bicentric study. They were identified in the records of the institutional head and neck cancer registry database. The EG was defined as patients aged 70 years or older and the YG as patients who were less than 70 years of age.
All of the patient electronic medical records were reviewed retrospectively to determine the clinical (age, tobacco and alcohol use, presence of oral lichen) and the disease (8th TNM stage, histological subtype, degree of differentiation, and prognostic features of SCC) pre-treatment parameters, the management details, and the outcomes. The treatments were decided in a multidisciplinary team meeting that took the patients’ comorbidities into account. Histological analysis and protocols treatments were done in each center.
The follow-up time was defined as the time between the histological diagnosis and the last follow-up or death. The causes of death were divided into two groups: related to the disease or independent of the disease. The causes linked to the disease included deaths related to recurrences, second localization in the upper aerodigestive tract, or due to the treatments. Deaths due to the treatment were defined as deaths during the treatment or within three months of the end of the treatment. The causes independent of the disease included cancers at sites other than the upper aerodigestive tract and non-carcinologic causes.
The descriptive analysis characterized the studied population in terms of frequencies, percentages, medians (min-max), and ranges. The variables were compared with Fisher’s exact test for the nominal qualitative data and the non-parametric Wilcoxon test for the ordinal qualitative data. Student’s test was used for the quantitative data. Survival times were defined as the time from the diagnosis to death or the last follow-up. OS was estimated using the Kaplan-Meier method and compared with the log-rank test. The survival curves were compared using the log-rank test for univariate analysis. The statistical analyses were performed using IBM SPSS Statistics for Windows, version 23 software (IBM Corp., Armonk, NY, USA). The significance threshold was p < 0.05.
Results
Between 2007 and 2017, 360 patients met the inclusion criteria and were included in the study. The median age was 69 years (range 37 - 94 years), 211 patients (59%) were male, and 149 (41%) were female. Tobacco use was identified in 183 out of 339 patients (55%) and a high level of alcohol consumption in 123 out of 327 (38%). Fifty-four patients (16%) had a medical history of head and neck cancer. The presence of lichen was assessed in 268 cases, and 26 of these (10%) were found to have lichen.
The group of younger patients included 190 patients with a median age of 59 years (min-max = 37-69) and the group of elderly patients included 170 patients with a median age of 79 years (min-max = 70-94). There were significantly more men in the YG and there were more women in the EG (p < 0.001). The patient characteristics and the tumor staging are presented in Table 1.
There was not a significant difference between the younger patients and the elderly patients in terms of the presence of lichen. There was significantly more tobacco and alcohol use in the younger group than in the elderly group (p < 0.001). A history of head and neck cancer was significantly more common in the younger patients than in the elderly patients (p = 0.002). The pharynx was the main previous localization in the younger group (23 out of 39) and the oral cavity for the elderly group (12 out of 15).
In both groups, classical SCC was the most common histology. There was not a difference in the tumor stage or the local histological characteristics between the two age groups, but a more advanced lymph node stage was significantly more common in the younger group (p = 0.01).
The repartition of the treatments is represented in Figure 1. Curative treatment was provided to 169 out of 190 patients (89%) in the YG, mainly as surgery with an adjuvant treatment, and to 138 out of 170 patients (81%) in the EG, mainly as surgery alone. In the curative group, the younger patients underwent significantly more adjuvant treatment after surgery than the elderly patients (p < 0.001).
There was not a difference in regard to differentiation, vascular embolus, perineural sheathing, capsular effraction, or the infiltration depth between the two age groups (Table 1).
Palliative treatment was provided to 21 patients (11%) in the YG and to 32 patients (19%) in the EG. In the YG, palliative treatment was provided due to the overall condition of the patient or due to an advanced stage of the disease, including metastasis. In the elderly group, palliative treatment was provided due to a poor overall condition; advanced disease, including metastasis; or other comorbidities that did not allow a curative treatment to be endured.
In the palliative group, the chemotherapeutic agents for the older patients were administered at doses adapted to take into account the age, as well as comorbidities and the general condition of the patients. The chemotherapy treatments were provided as monotherapies (methotrexate or paclitaxel) or as bitherapies (docetaxel, 5-fluorouracil, cetuximab, carboplatin).
The median follow-up was 37 months (min-max = 0-133) in the YG and 24 months (min-max = 0-130) in the EG, considering all treatment types. There was not a significant difference in the OS between the two age groups (p = 0.051 – Figure 2).
The five-year OS was 53% for the younger patients and it was 46% for the elderly patients. At the last follow-up, 87 patients (46%) of the YG had died and 82 patients (48%) of the EG had died. There was not a significant difference in the causes of death between the two age groups (Figure 3).
In the curative group, there was not a difference in the OS between the two age groups (p=0.1). At the last follow-up, 72 out of 169 patients (43%) in the YG were deceased and 62 out of 138 patients (45%) in EG were deceased. In these cases, 43 out of 72 of the deaths (60%) were related to the disease in the YG, including 7 out of 72 (10%) related to the treatment. In the EG, 39 out of 62 of the deaths (63%) were related to the disease, of which 18 out of 62 (29%) were related to the treatment. There were significantly more deaths related to the treatment for the EG than for the YG (p = 0.007).
In the palliative treatment EG, the median follow-up period was 13.5 months (min-max = 1-71) and six of the sixteen patients treated by chemotherapy had a survival that was longer than 24 months. In the palliative treatment YG, the median follow-up was 13 months (min-max = 3-119) and seven of the twenty patients treated by chemotherapy had a survival that was longer than 24 months.
In the curative group, the DFS was significantly better for the YG than for the EG (p = 0.02). The five-year DFS was 53% for the YG and 39% for the EG (Figure 4).
After curative treatment, recurrences occurred in 66 out of 169 of the patients (39%) in the YG and in 50 out of 138 of the patients (36%) in the EG. The frequency and the localizations of the recurrences are indicated in Table 2. There were 38 out of 66 recurrences (58%) in the YG that resulted in death, while 21 out of 50 of the recurrences (42%) in the EG resulted in death. For the EG, the presence of lichen was associated with more local recurrences (p = 0.019), unlike the YG, for which the presence of lichen was not associated with an increase in local recurrences (p = 0.08).
Table 1: The patient and the tumor characteristics.
| Younger group | Elderly group | p | ||
|---|---|---|---|---|
| Number | n=190 (53%) | n=170 (47%) | ||
| Median age (range) | 59 (min-max=37-69) | 79 (min-max=70-94) | ||
| Gender | Male (n=211) | n=132(69%) | n=79(46%) | <0.001 |
| Female (n=149) | n=58 (31%) | n=91 (54%) | ||
| Tobacco | No (n=148) | n=43 (23%) | n=105 (67%) | <0.001 |
| Yes (n=191) | n=140 (77%) | n=51 (33%) | ||
| Alcohol | No (n=204) | n=77 (44%) | n=127 (83%) | <0.001 |
| Yes (n=123) | n=97 (56%) | n=26 (17%) | ||
| Tobacco and alcohol | No (n=211) | n=79 (46%) | n=132 (86%) | <0.001 |
| Yes (n=116) | n=95 (54%) | n=21 (14%) | ||
| Previous head and neck cancer | No (n=303) | n=149 (79%) | n=154 (91%) | 0.002 |
| Yes (n=54) | n=39 (21%) | n=15 (9%) | ||
| Histology | Classical (n=335) | n=181 (95%) | n=154 (91%) | 0.75 |
| Verrucous (n=22) | n=7 (4%) | n=15 (9%) | ||
| Sarcomatoid (n=3) | n=2 (1%) | n=1 (1%) | ||
| Differentiation | Limited or moderate(n=59) | n=28 (16%) | n=31 (20%) | 0.32 |
| Pronounced (n=268) | n=147 (84%) | n=121 (80%) | ||
| Vascularembolus | No (n=190) | n=104 (83%) | n=86 (86%) | 0.58 |
| Yes (n=35) | n=21 (17%) | n=14 (14%) | ||
| Perineural sheathing | No (n=134) | n=80 (63%) | n=54 (55%) | 0.22 |
| Yes (n=91) | n=46 (37%) | n=45 (45%) | ||
| Capsular effraction | No (n=298) | n=153 (81%) | n=145 (88%) | 0.11 |
| Yes (n=55) | n=35 (19%) | n=20 (12%) | ||
| Infiltration depth | Average, in mm | 10.88 | 11.41 | 0.84 |
| T stage | Tis – T2 (n=82) | n=43 (23%) | n=39 (24%) | 0.89 |
| T3 – T4 (n=271) | n=146 (77%) | n=125 (76%) | ||
| N stage | N0 – N2a (n=156) | n=126 (67%) | n=130 (79%) | 0.01 |
| N2b – N3b (n=97) | n=62 (33%) | n=35 (21%) |
Table 2: Distribution of the recurrences. Abbreviations: YG, younger group; EG, elderly group.
| YG | EG | n=66/169 (39%) | n=50/138 (36%) |
|---|---|---|
| Locoregional | n=46 (70%) | n=41 (82%) |
| Metastatic only | n=11 (17%) | n=8 (16%) |
| Local or lymph nodes and metastatic | n=9 (13%) | n=1 (2%) |
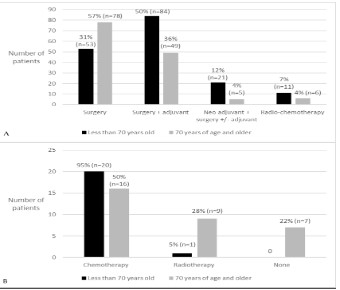
Figure 1: Treatments by age (A: curative, B: palliative).
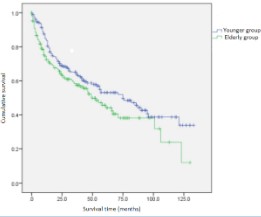
Figure 2: Overall survival, considering all treatments.
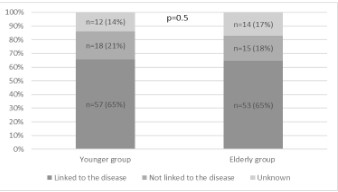
Figure 3: Distribution of causes of deaths.
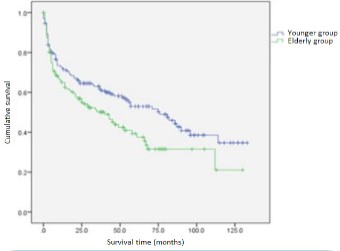
Figure 4: Disease-free survival, considering curative treatments.
Discussion
Elderly and younger patients differ in terms of the clinical presentation of gingival SCC. In elderly patients, the disease mainly affects women [10], non-smokers, and non-drinkers, whereas in younger patients men more often have an oral cavity localization [11]. Our study confirms these demographic differences in the gingival localization. Dahlstrom et al. also dem- onstrated that the gingiva is the most frequent localization of head and neck SCC in women over 70 years of age who do not smoke or drink alcohol [9].
The incidence of oral squamous cell carcinoma increases with age and the presence of oral lichen [12]. Our study found an increase in local recurrences and second buccal localizations in elderly patients who also had oral lichen. These findings suggest that a mucosa modification process linked to age could be an independent risk factor of gingival SCC.
The tumor characteristics also appear to differ according to the age of the patients. Even with locally advanced tumors, our study found a decrease in nodal involvement in the EG versus the YG, suggesting less aggressive tumors in the EG despite the absence of histological differences for local tumors. This has been described in head and neck SCC, albeit not specifically in oral SCC [13].
Funk et al. also reported different histological characteristics, with an increase in verrucous SCC compared to classical SCC in the elderly [8]. The histological type and the differentiation in our study did not differ between the two age groups.
In the curative group, the elderly patients less often received adjuvant treatments. The criteria for adjuvant treatment were the same for the whole population, and this difference can be due to two reasons: less indication of adjuvant treatments linked to lower nodal involvement, or an overall condition incompatible with adjuvant treatment in postoperative elderly patients. Sanabria et al. found that elderly patients suffered from suboptimal treatment without adjuvant treatment, as it decreased DFS, but there was no difference in overall survival in their study [14].
In our study, the difference in OS was at the limit of significance between the two age groups considering all treatment types. In the curative group, there was not a significant OS difference between the two groups, but the DFS was also decreased in the EG, even though the frequency and the localization of recurrences were similar in the two age groups. The decreased DFS in the EG can be explained by the higher rate of different events in the EG than in the YG. There was not a difference in the number of deaths linked to the disease between the two age groups, but there were more deaths due to the treatments in the EG. There was not a difference in the rate of recurrences between the two age groups, although there were fewer deaths due to recurrences in the EG than in the YG.
Surgery is the standard treatment for gingival carcinoma. Of note, a quarter of the deaths linked to the disease in the elderly are due to the treatment. Moreover, in the palliative group, 6 out of 16 of the elderly patients receiving a customized chemotherapy were long-term survivors (more than two years).
These results suggest that local control need not always be the rule with these types of tumors. The risk-benefit ratio should be considered to avoid undertreatment and iatrogenic events. Surgery remains the gold standard for treatment, although it is not necessarily always the best option. Local control with multiple surgeries could be replaced with chemotherapy to preserve quality of life in some elderly patients who have less aggressive tumors that could involve mucosa degeneration with a different disease progression. Thus, chemotherapy could be a suitable alternative in selected elderly patients. Geriatric evaluation is essential to decide what medical care is indicated: a standard treatment, a customized treatment, or a symptomatic treatment.
Conclusion
Gingival mandibular SCC in elderly patients appears to be a different entity than other oral SCC, involving more women, non-smokers, and non-drinkers. These SCC appear to be less aggressive, with less nodal extension, even though they are locally advanced at the time of diagnosis. Surgery remains the gold standard for treatment, but soft chemotherapy appears to be a good alternative in elderly patients with gingival mandibular SCC with high comorbidities who cannot undergo major surgery. Local control should not always be considered the treatment of choice in this population at risk of greater toxicity to treatments. Evaluation is essential to tailor the treatment to each elderly patient.
Conflict of interest: Authors have no conflict of interest.
References
- Gorphe P, Guerlain J, Moya-Plana A, Janot F, Even C, et al. Epidémiologie des cancers des VADS chez les patients âgés en France. 51st French cervico-facial carcinology society congrest. 2018; France. Brest, 2018.
- Jelinek MJ, Howard AS, Haraf DJ, Vokes EE. Management of Early Head and Neck Cancer in Elderly Patients. J Oncol Pract. 2018; 14: 541-546.
- Yap T, McCullough M. Oral medicine and the ageing population. Aust Dent J mars. 2015; 60: 44-53.
- Wael Youssef E. Age-Dependent Differential Expression of Apoptotic Markers in Rat Oral Mucosa. Asian Pac J Cancer Prev. 2018; 19: 3245-3250.
- Ashcroft GS, Mills SJ, Ashworth JJ. Ageing and wound healing. Biogerontology. 2002; 3: 337-345.
- Malaguarnera L, Cristaldi E, Malaguarnera M. The role of immunity in elderly cancer. Crit Rev Oncol Hematol. 2010; 74: 40-60.
- Swango PA. Cancers of the oral cavity and pharynx in the United States: an epidemiologic overview. J Public Health Dent. 1996; 56: 309-318.
- Funk GF, Karnell LH, Robinson RA, Zhen WK, Trask DK, Hoffman HT. Presentation, treatment, and outcome of oral cavity cancer: a National Cancer Data Base report. Head Neck. 2002 ; 24: 165-180.
- Dahlstrom KR, Little JA, Zafereo ME, Lung M, Wei Q, Sturgis EM. Squamous cell carcinoma of the head and neck in never smokernever drinkers: a descriptive epidemiologic study. Head Neck. 2008 ; 30: 75-84.
- Italiano A, Ortholan C, Dassonville O, Poissonnet G, Thariat J, et al. Head and neck squamous cell carcinoma in patients aged > or = 80 years: patterns of care and survival. Cancer. 2008 ; 113 : 3160-3168.
- Pires FR, Ramos AB, Oliveira JBC de, Tavares AS, Luz PSR da, et al. Oral squamous cell carcinoma: clinicopathological features from 346 cases from a single oral pathology service during an 8-year period. J Appl Oral Sci. 2013; 21: 460-467.
- Laniosz V, Torgerson RR, Ramos-Rodriguez AJ, Ma JE, Mara KC, et al. Incidence of squamous cell carcinoma in oral lichen planus: a 25-year population-based study. Int J Dermatol. 2019; 58: 296-301.
- Malik A, Mishra A, Chopda P, Singhvi H, Nair S, et al. Impact of age on elderly patients with oral cancer. Eur Arch Otorhinolaryngol. 2019; 276: 223-231.
- Sanabria A, Carvalho AL, Vartanian JG, Magrin J, Ikeda MK, et al. Factors that influence treatment decision in older patients with resectable head and neck cancer. Laryngoscope. 2007; 117: 835-840.